
What to Know About Peer Coaching in NH
Learn how peer coaching NH supports recovery with state credentialing, Medicaid coverage, and resources for seamless aftercare and virtual options.
June 1, 2026


Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
You already know the shape of your week. Standing meetings, a commute that eats both ends of the day, a calendar that other people fill in faster than you can clear it. Somewhere inside that schedule, you're trying to deal with a drinking pattern that crept up on you, or a prescription that became something else, or a quiet anxiety you've been managing with whatever works. You don't need a brochure. You need to know whether real treatment can fit inside the life you've built without flattening it.
Holistic virtual care, as it's actually practiced in Connecticut, is built around a few non-negotiables for someone in your position. It treats the substance use and the mental health piece together, not in separate clinics with separate wait times. It includes medication when medication helps, not as a last resort. It runs on hours that exist outside the 9-to-5, and it happens on a screen in a room you control.
It's also clinically grounded here. The state's Department of Mental Health and Addiction Services frames co-occurring care as phased, recovery-oriented, and integrated, not as wellness add-ons stapled to a detox protocol. That definition matters because it's the standard Connecticut programs are measured against. The rest of this guide walks through what that looks like in practice, what your insurance and the state's policy framework actually cover, and how to tell a serious program from a polished landing page.5

If you've been quietly wondering whether you're the only person in Connecticut juggling a job, a household, and a substance use issue, the state's own numbers will tell you something different. In fiscal year 2024, the Department of Mental Health and Addiction Services (DMHAS) served roughly 46,405 unduplicated individuals across its substance use programs, with 46,236 admissions and a 6.4% year-over-year increase in admissions. That growth isn't a sign that things are falling apart. It's a sign that more people are reaching for treatment, and that the system is being asked to meet them.4
Those figures count people who entered DMHAS-funded or DMHAS-affiliated services. They don't include everyone treated through commercial insurance, private practices, or employer assistance programs, so the real population of Connecticut adults working on a substance use issue is larger than what the report shows. If you're insured through your employer and have never touched the public system, you're not in that 46,405. You're somewhere alongside it.
What the climb in admissions also tells you is that capacity is expanding to match demand. Programs are adding evening and early-morning hours. Telehealth slots are being treated as standard, not as overflow. The state's investment posture, which the next sections cover in detail, has shifted toward keeping people in care rather than measuring whether they qualify for it. For someone in your position, that translates into shorter waits and more flexibility about when and how you start. The growth in the chart below isn't an abstract policy story. It's the reason a Tuesday-night intake appointment is a real option this month instead of a six-week wait.
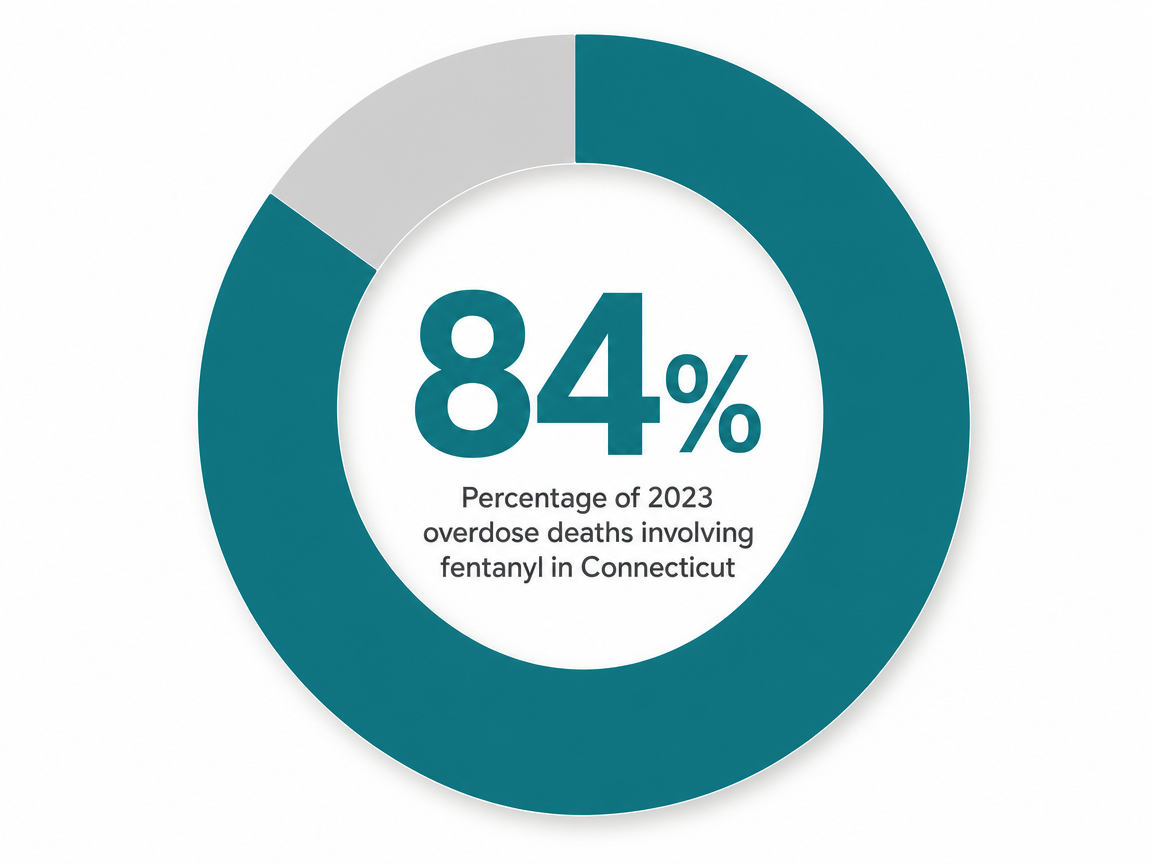
Public conversation about addiction in Connecticut tends to default to opioids, and there's a reason for that. More than half of DMHAS clients have a substance use disorder, with opioid-related diagnoses the most frequent, and the FY25 statistical report logged 18,858 heroin and other opioid cases. Fentanyl is the driver behind most of the harm. The Connecticut Opioid Response (CORE) Initiative documents fentanyl presence in 84% of 2023 overdose deaths, an unforgiving statistic that explains why medication for opioid use disorder is treated as a first-line clinical tool rather than a last resort.1,13
That story is real, and it's not the whole story. DMHAS data on the broader landscape shows alcohol remains the substance of highest use prevalence in Connecticut, and SUD-related emergency department visits ran at 338.1 per 100,000 in 2023. If your concern is a drinking pattern that quietly doubled during a stretch of overtime, you are inside the largest part of the picture, not the margins of it.12
What ties these threads together is how often a substance use issue arrives with something else along for the ride. Anxiety. Depression. Insomnia that turned into a wine habit. ADHD that got treated with stimulants you stopped controlling. The case for integrated, holistic care isn't ideological. It's practical. Treating the substance use without the mood disorder, or the mood disorder without the substance use, tends to leave the half you didn't address to undo the half you did. That's exactly the gap Connecticut's co-occurring program guidelines are written to close, and it's the gap a well-built virtual program is designed to hold both sides of at once.
The word "holistic" gets stretched in marketing copy until it loses meaning. In Connecticut, you actually have a clinical definition to anchor it. The state's Co-Occurring Enhanced and Co-Occurring Capable Program Guidelines, written and maintained by DMHAS, lay out what integrated care for substance use and mental health is supposed to look like. Programs are evaluated against those guidelines. So when a Connecticut clinician calls a program holistic, the word should map to something specific.
The guidelines build around a few principles you can hold in your head. Care is phased, meaning what you need in week two is different from what you need in month four, and the program adjusts to where you actually are. It uses a recovery perspective, which means the goal is a life you want to live, not just abstinence as a metric. It addresses cognitive impairments and trauma rather than treating them as someone else's problem. And it incorporates families in the recovery process, on the assumption that the people closest to you have a role in what gets better and what stays hard.5,7
What that means for you, practically: a program that takes the guidelines seriously will not hand you a generic curriculum and a 12-step meeting schedule. It will assess where you are, treat the substance use and the anxiety or depression in the same plan, and adjust as you move through stages. "Holistic" in this frame is a structure, not a vibe.
If you map the DMHAS phased, recovery-oriented co-occurring approach onto a virtual delivery model, you get a fairly concrete list of parts. None of them are optional, and none of them stand alone. The point is how they fit together.5
Medication for addiction treatment sits at the center for many people, especially if your concern is opioids or alcohol. That includes buprenorphine and Suboxone for opioid use disorder, naltrexone for alcohol or opioid use, and psychiatric medication management for the anxiety, depression, or sleep issues riding alongside. A prescriber meets with you on video, reviews labs, adjusts doses, and stays available between visits. Medication is treated as a clinical tool, not a moral compromise.
Virtual intensive outpatient (IOP) is the structural backbone for a lot of working adults. You meet in a small group several evenings or mornings a week for a defined stretch of weeks. Individual therapy runs in parallel, usually weekly, with a clinician who knows your full picture. Group therapy adds the part you cannot get from one-on-one work: hearing other people in recovery describe the exact thing you thought only you were doing.
Peer recovery coaching brings someone with lived recovery experience into your week, usually outside clinical hours, to help with the practical scaffolding. Mindfulness-based cognitive therapy and other evidence-based modalities give you tools for the moments between sessions, when a craving or a panicked Tuesday at 4 p.m. hits and you need something to do with your hands and your attention.
Family support and co-occurring mental health treatment round it out. Family work, when you choose to include it, helps the people around you stop unintentionally undoing the work you're doing. Co-occurring care means the same team treating the substance use is also treating the depression or anxiety alongside it, in one coordinated plan rather than two parallel ones that never speak. Holistic, in this clinical sense, is the assembly. Not any one piece.7
Honest expert guidance includes the limits. Virtual holistic care covers a wide arc, but it does not cover everything, and pretending otherwise would put you in a worse spot than you started.
If you're physically dependent on alcohol or benzodiazepines at a level where withdrawal carries real medical risk, you need supervised detox before, or alongside, virtual programming. Some at-home and ambulatory detox protocols work well with telehealth oversight. Others require a higher level of medical monitoring than a screen can provide. A good intake will tell you which side of that line you're on.
Acute psychiatric crisis is the other limit. If you're in a mental health emergency, in active danger, or experiencing symptoms that require inpatient stabilization, that's primary psychiatric care, and it belongs in a setting equipped for it. Virtual co-occurring treatment is built to integrate with mental health care once you're stable, not to replace crisis services.
The point isn't to talk you out of virtual care. For most working professionals managing a substance use issue with anxiety or depression alongside, this delivery model fits well. It's to make sure that if you do start virtually, you're starting at a level of care that matches what's actually going on.
It's worth knowing that the version of virtual care you can access in Connecticut today did not exist a few years ago in the same form. Two policy moves did most of the work to make it real, and both of them sit underneath whatever program you eventually pick.
The first is the Section 1115 SUD demonstration waiver, approved on April 14, 2022, which gave Connecticut Medicaid the authority to cover the full continuum of substance use care, including residential and inpatient levels of treatment delivered or supported through telehealth. The 2025 mid-point assessment confirmed the waiver is still in place and being measured against its goals. What that means in plain terms: the state is no longer treating telehealth as a workaround for in-person care. It's a covered, evaluated piece of the continuum.10
The second is the HUSKY MAT benefit. CMS approved Connecticut's state plan amendment (CT-25-0040) to make medication for addiction treatment a permanent, mandatory Medicaid benefit with no end date, transferring MAT provisions into the state plan in line with the federal SUPPORT Act. If you're insured through HUSKY, MAT delivered virtually, including the prescriber visits and the medication itself, is not a temporary pilot. It's standard coverage.3
For someone with commercial insurance, those Medicaid changes still matter. They set the floor that private plans tend to follow, and they shaped the provider network you'll be choosing from.
Policy authority is one thing. Money to actually build out the programs is another, and Connecticut has been moving on both at once.
In January 2025, Governor Lamont announced a $58.6 million investment to create a program providing access to substance use disorder treatment services, drawn from the state's broader opioid settlement work. Connecticut has secured roughly $600 million in opioid settlement funds, part of the $50 billion in national settlements the state helped lead. Then in May 2025, the Opioid Settlement Advisory Committee allocated $10,050,000 specifically for Opioid Treatment Program access expansion, money pointed directly at adding capacity, including the kind of MAT capacity that virtual programs depend on. Those two figures, side by side, tell you the funding direction is not a single press release. It's a sustained build-out.2,8
That money flows down. The 2025 municipal opioid settlement expenditure report shows towns across Connecticut allocating their share to local health departments and SUD initiatives, which seeds regional capacity even when you never see the headline. On top of settlement dollars, DMHAS pulls in annual federal block grants from SAMHSA, including the Community Mental Health Services and Substance Use Prevention, Treatment, and Recovery Services block grants, totaling over $30 million in a typical year. Those grants are the quiet backbone that keeps slots open at sliding-scale rates.6,11
What this looks like for you: shorter waitlists, more evening and weekend telehealth slots, and programs willing to take a wider range of insurance plans because their revenue mix is healthier than it used to be. The infrastructure under your appointment is finally catching up to the demand sitting on top of it.
The fastest way to picture this is to lay it over a real week. Virtual intensive outpatient programs in Connecticut typically run nine to twelve clinical hours a week, structured as group sessions a few days a week plus individual therapy and a medication visit. The hours are deliberately built around people who work.
A common pattern: group therapy three evenings a week, roughly 5:30 to 8:30 p.m., with one individual therapy session slotted into a lunch hour or a late afternoon. Medication management with a prescriber happens monthly or twice a month, in a 20- to 30-minute video visit you can take from your office with the door closed. Peer recovery coaching often lives outside that frame entirely, a Saturday morning call or a weeknight check-in that doesn't compete with your meeting load.
What disappears from the picture is the hour you used to spend driving to a clinic and the hour back. That alone is the difference between treatment being possible and being theoretical for someone with a full calendar. The 1115 SUD demonstration waiver makes this configuration a covered piece of Connecticut's continuum, not a workaround.10
Yes, three evenings a week sounds like a lot when you read it on paper. It is. It's also a defined stretch, usually eight to twelve weeks at the IOP level, after which the intensity steps down. You're not signing up for forever. You're signing up for a season where you put the substance use issue at the front of the line, then you transition to a lighter cadence as things stabilize. That phased structure is exactly what the DMHAS guidelines describe.5
Privacy is usually the first question, even when it's the second one asked. Here's the plain version.
If you pay for treatment through your insurance, your employer does not see your diagnosis or your session notes. Your insurer does, because they're paying claims, but federal law sharply limits what flows back to your employer. Group health plans receive aggregated cost data, not individual records. HR doesn't get a memo when you start a virtual IOP.
What your employer might see is time. If you need to protect three evenings and a lunch hour for a stretch of weeks, you have a few options. Many people do virtual IOP without ever telling their employer, because the hours fit around the workday. If you need formal protection, the Family and Medical Leave Act covers substance use treatment as a serious health condition, and you can request intermittent FMLA leave through HR or a third-party administrator without disclosing the specific diagnosis to your manager. The certifying clinician handles that paperwork.
One practical note. Take video sessions from a private space, not a shared office or an open conference room. A locked door and headphones do most of the work.
Not every program calling itself holistic is built the same way. A short list of questions will tell you most of what you need to know on a fifteen-minute intake call.
Ask whether the program is co-occurring capable or co-occurring enhanced under the DMHAS framework, and what that means for how they treat anxiety, depression, or trauma alongside the substance use. A serious program will answer in specifics, not adjectives. Ask whether your therapist and your prescriber are on the same team and share notes, or whether you'd be coordinating two separate practices yourself. Integrated care means one plan, one team.5,7
Ask about medication. If you're considering buprenorphine, Suboxone, or naltrexone, the prescriber should be available within days of intake, not weeks. With HUSKY MAT now a permanent Medicaid benefit and commercial plans largely following suit, there's no policy reason for a long wait.3
Ask about hours. Specifically, ask what evening and early-morning slots exist, and whether group times are fixed or flexible. Ask how they handle a week where you travel for work.
Ask about family involvement, on your terms. Connecticut's co-occurring guidelines treat family inclusion as part of recovery, not an optional extra, but you decide what that looks like for you.7
Last, ask what they do not treat. A program that names its limits is one you can trust on the things it does take on. If you'd rather start with a Connecticut-licensed virtual program built specifically for working adults, Pathfinder Recovery is one option to put on your shortlist.
If you or a loved one are ready to create a life you love—without having to sacrifice your work, family, and responsibilities—we're here to support you on that journey. Contact us today for personalized care from the comfort of your own home. We will work with your insurance provider so you can focus on what really matters: recovery.
Yes, in most cases. HUSKY (Connecticut Medicaid) now covers medication for addiction treatment as a permanent, mandatory benefit with no end date, including virtual delivery. The state's 1115 SUD demonstration waiver also extends coverage across the full continuum of care, including telehealth-supported levels. Commercial plans generally follow that floor. When you call a program, ask them to verify your specific plan before your first session.3,10
Yes. A Connecticut-licensed prescriber can evaluate you over video, prescribe buprenorphine, Suboxone, or naltrexone, and manage your doses through ongoing telehealth visits. Labs get ordered locally, and prescriptions go to your pharmacy. With HUSKY MAT now a permanent Medicaid benefit aligned with the federal SUPPORT Act, virtual MAT is standard coverage, not a pilot. A serious program will get you in front of a prescriber within days of intake.3
Not from your insurance. Group health plans receive aggregated cost data, not individual diagnoses or session notes. Your manager doesn't get notified when you start treatment. The visible piece is time, the evening or lunch hours you protect. Many people keep IOP entirely private. If you need formal job protection, the Family and Medical Leave Act covers substance use treatment, and your clinician handles the paperwork without disclosing the diagnosis to your manager.
Weekly therapy is one piece. Holistic virtual care assembles several, working together: medication management, group therapy a few evenings a week, individual sessions, peer recovery coaching, and co-occurring mental health treatment in one coordinated plan. DMHAS frames this as phased, recovery-oriented integrated care, not a single appointment on your calendar. The structure is what makes it clinically holistic, not the addition of wellness language to a weekly check-in.5,7
That's the rule, not the exception, and it's exactly what co-occurring care is built for. Connecticut's Co-Occurring Capable and Enhanced Program Guidelines require that programs treat both conditions in one integrated plan, with the same team handling the substance use and the mental health piece. You won't be sent to two separate clinics that don't talk. One assessment, one plan, one team adjusting both sides as you move through stages.5,7
Virtual care covers a wide range, but not everything. If you're physically dependent on alcohol or benzodiazepines at a level where withdrawal carries medical risk, you need supervised detox, sometimes inpatient, before or alongside virtual programming. If you're in an acute psychiatric crisis or active danger, that's primary psychiatric care in a setting equipped for it. A good intake will tell you which level you're at and help connect you to the right starting point.
June 1, 2026

February 6, 2026
