Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
Key Takeaways
Virtual rehab is real treatment, offering medical detox support, MAT, intensive outpatient groups, individual therapy, peer coaching, and co-occurring mental health care delivered by licensed clinicians through video.
Outcomes hold up against in-person care, with telemedicine retention reaching 50% versus 39% for traditional treatment at one year and comparable abstinence results.1
SAMHSA made 2024 telehealth flexibilities permanent, letting prescribers start buprenorphine by video without an initial in-person exam, expanding access for rural and transportation-limited patients.5
Online rehab is the wrong fit during severe withdrawal with seizure history, psychiatric crisis, unsafe home environments, or repeated outpatient relapse, where higher levels of care are needed first.
The Short Answer, Before You Close This Tab
Yes. You can go to rehab online, and it counts as real treatment.
If you are in Vermont, Massachusetts, Connecticut, or New Hampshire, a fully virtual program can give you medical detox support at home, prescription medication for alcohol or opioid use disorder, intensive outpatient group therapy, individual counseling, peer coaching, and care for the anxiety or depression that often rides alongside substance use. You meet your clinicians by video. You take medication that a licensed prescriber sends to your pharmacy. You sit in group from your kitchen table, your car on lunch break, or your bedroom after the kids are asleep.
This is not a wellness app or a chat box. Telehealth for substance use disorders is recognized as evidence-based practice by SAMHSA, the federal agency that sets the standard for addiction care in the United States. The research base is real, the medications are the same ones used in residential programs, and the clinicians on the other side of the screen are licensed in your state.4
If that is what you came here to find out, you have your answer. The rest of this guide walks you through what virtual rehab actually includes, what it cannot do, and how to tell whether it fits your life this week.
What Counts as Real Virtual Rehab
When people picture rehab, they picture a building. A bed in a shared room. A schedule taped to a wall. Real virtual rehab keeps almost everything that happens inside that building and removes the building.
Here is what a full virtual program actually includes:
Medical detox support at home. A licensed clinician assesses whether you can withdraw safely outside a hospital, then monitors you by daily video and phone check-ins, with prescription medications to ease symptoms.
Medication for addiction treatment (MAT). A prescriber meets with you by video, evaluates whether buprenorphine, naltrexone, or another medication fits your situation, and sends the prescription to your pharmacy. Follow-up visits happen on the same screen.
Intensive outpatient programming (IOP). Group therapy, several times a week, usually nine to twelve hours total, run by licensed counselors. You log in, you participate, you do the work. It is the same clinical model as in-person IOP, just delivered through a secure video platform.
Individual therapy. One-on-one sessions with a licensed therapist who knows your history, your triggers, and the people in your life by name.
Peer recovery coaching. Time with someone who has lived through their own recovery and can tell you what worked at week three, month six, year two.
Co-occurring mental health care. If anxiety, depression, or trauma are tangled up with the substance use, treatment for those conditions is built into the same program rather than handed off to a separate clinic.
Family support. Sessions and resources for the people who have been worrying about you, often for longer than you realize.
SAMHSA, the federal agency that publishes the playbook for addiction treatment in the United States, recognizes telehealth-delivered SUD care across this full continuum as evidence-based practice, with specific implementation guidance for adult populations. That matters because it means virtual rehab is not a lighter version of treatment for people who could not get a real bed. It is treatment, designed and studied as such.4
What you should not call virtual rehab: a meditation app, a single weekly therapy session, or a chatbot that suggests coping skills. Those tools have their place, but they are not a program. A program has clinicians, medication when you need it, structure across the week, and a plan that changes as you do.
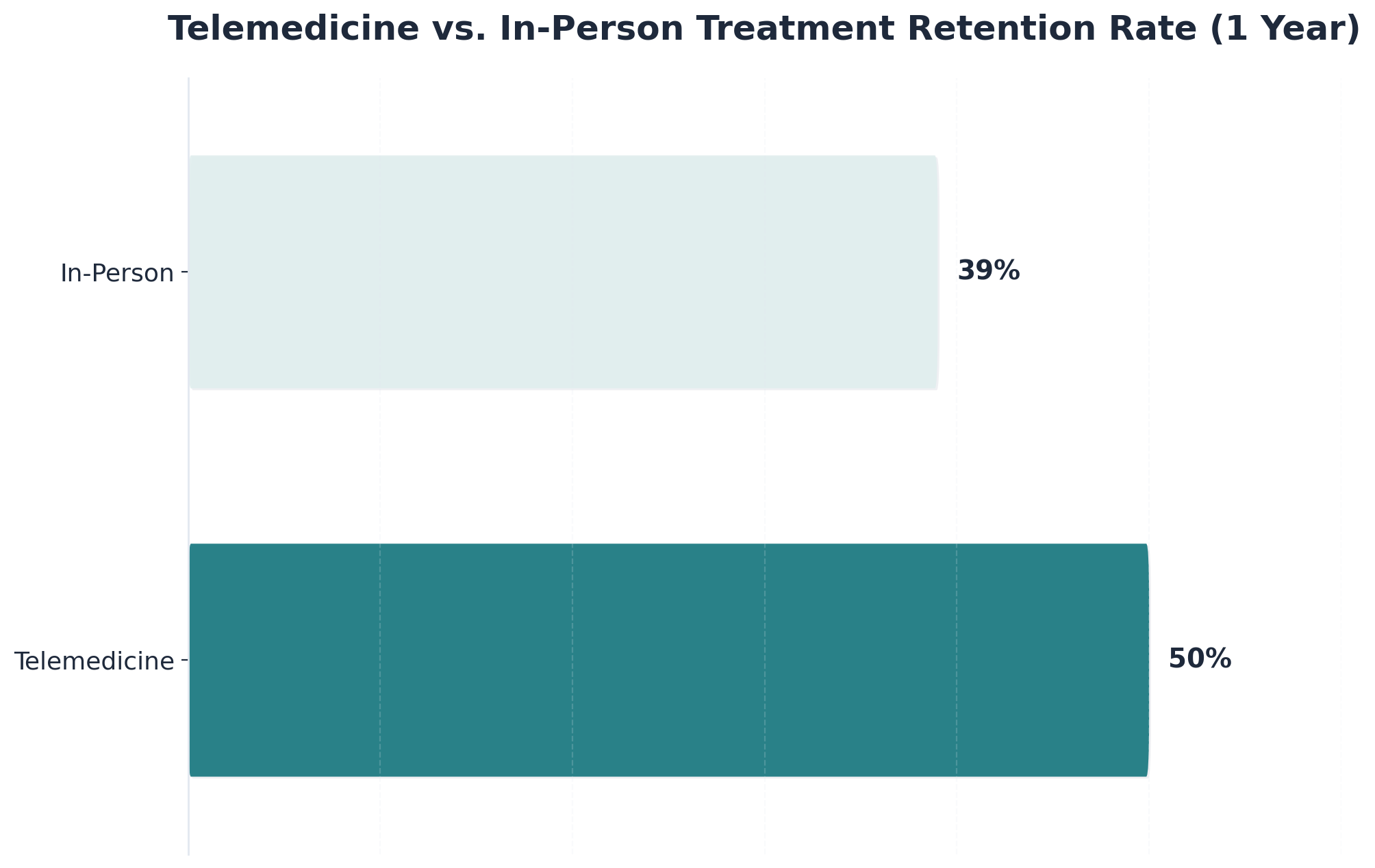
Telemedicine vs. In-Person Treatment Retention Rate (1 Year): Telemedicine: 50%, In-Person: 39%. A comparison of patient retention rates after one year for telemedicine-based substance use disorder treatment versus traditional in-person treatment.
Does It Actually Work? The Evidence Worth Knowing
This is the question that probably brought you here. If you are going to log in from your living room instead of checking into a building for thirty days, you want to know the outcomes hold up.
They do.
The clearest evidence comes from a systematic review that pooled 19 studies covering roughly 3,000 patients in treatment for opioid, alcohol, and tobacco use disorders. At one year, retention in care was 50% for patients treated by telemedicine, 47% for hybrid programs that mixed virtual and in-person visits, and 39% for traditional in-person treatment. Abstinence outcomes across the three groups showed no significant differences. Put plainly: people stuck with virtual care at least as well as they stuck with going to a clinic, and often better.1
Retention matters more than it sounds. Staying in treatment is one of the strongest predictors of whether someone stops using, stays stopped, and rebuilds the parts of life that addiction took. A program you can actually keep showing up to is better than a program you cannot.
The rest of the evidence base points the same direction. A 2025 meta-analysis found that remote and digital interventions reduced relapse and the number of days people used substances, particularly when added to a continuum of care. A study of the VA's video telehealth tablet program found that giving patients the technology increased the frequency of substance use disorder psychotherapy and group visits, rather than letting attendance slip. Virtual intensive outpatient programs have shown higher attendance and stronger engagement than traditional in-person IOP in feasibility research.3,7,9
There are honest limits worth naming. The research base is heterogeneous, meaning studies differ in how they delivered care and what they measured, and some questions about the most severe cases of substance use disorder are still being studied. Hybrid models, where you do most things virtually but occasionally see someone in person, often perform best of all.6
What the evidence does not show is the thing many people fear: that virtual treatment is a worse version of the real thing. It is not. For most adults with substance use disorders, it is the real thing, with a screen instead of a commute.
Detox at Home: What Virtual Care Can and Cannot Do
Detox is the part people are most afraid of, and most ashamed to ask about. The honest answer: a lot of it can happen at home, with the right support. Some of it cannot, and a good program tells you which is which on the first call.
For many people withdrawing from alcohol or opioids, ambulatory detox, meaning detox you go through while still living your life, is a clinically reasonable option. A licensed prescriber evaluates your history, how much you have been using, how long, any seizures or DTs in the past, your medical conditions, and what is going on at home. If you are a candidate, they prescribe medications to ease withdrawal, set up daily video check-ins, and put a phone line in your pocket for the rough hours.
This kind of remote monitoring is not improvised. A VA study of telehealth-supported detox found that low-cost phone monitoring during and after detox reduced repeat detox episodes, meaning people were less likely to keep cycling back through withdrawal again and again. Staying connected during the hardest week is part of what makes the next week possible.10
What virtual detox cannot do: handle a medically complex withdrawal that needs IV fluids, cardiac monitoring, or a hospital bed. Severe alcohol withdrawal with seizure history, benzodiazepine withdrawal at high doses, pregnancy, unstable heart conditions, or a home that is not safe to detox in, those situations need a higher level of care. A responsible virtual program will tell you that directly and help you find the right setting, not push you into a model that does not fit.
If you are not sure which category you are in, that is exactly what the intake assessment is for. You do not have to diagnose yourself before you call.
Medication for Addiction: Buprenorphine, Naltrexone, and the 2024 Rule Change
If your substance use involves opioids or alcohol, medication is probably going to be part of the conversation. That is not a failure or a shortcut. It is the standard of care, and the medications work. Buprenorphine quiets opioid cravings and withdrawal without the high. Naltrexone, available as a daily pill or a monthly injection, blocks the reward from alcohol and opioids so that drinking or using stops doing what it used to do. Both have decades of research behind them and both can now be prescribed, started, and managed entirely by video visit.
That last part is newer than most people realize. For years, buprenorphine prescribing was tangled in a federal requirement that the first appointment had to happen in person. The rule loosened during COVID as a temporary emergency flexibility, and a lot of people assumed it would snap back. It did not. In 2024, SAMHSA made those telehealth flexibilities permanent, allowing clinicians to evaluate and start patients on buprenorphine through a video visit, without an initial in-person exam. The same rule expands access for people in rural areas, people without transportation, and people who cannot or will not walk into a clinic with a sign on the door.5
The practical effect is straightforward. You schedule an intake. A licensed prescriber meets you on video, takes your history, talks through what you have been using and how often, and decides with you whether buprenorphine, naltrexone, or another medication is the right starting point. If buprenorphine is the plan, the prescription goes to your pharmacy that day or the next. You pick it up like any other medication. Follow-up visits, dose adjustments, and check-ins all happen on the same screen.
Naltrexone has always been easier to prescribe by telehealth because it is not a controlled substance, but the rhythm of care is similar. A prescriber, a plan, regular visits to see how you are doing, and a phone number for the days when something feels off.
What virtual MAT does not do is hand you a prescription and disappear. The medication is one piece. The therapy, the group, the peer coach, the family work, those are the structure that keeps the medication doing its job. Pathfinder pairs MAT with virtual IOP and counseling for exactly that reason, across Vermont, Massachusetts, Connecticut, and New Hampshire.
Recovery, Made Possible — From Home
Pathfinder Recovery offers in-home addiction and mental health treatment that fits your life — not the other way around.From at-home detox and MAT to virtual IOP and peer support, our licensed clinicians bring evidence-based care to you through secure telehealth.
A Week in Virtual IOP: Tuesday Group, Thursday Prescriber, Sunday Reset
Abstract schedules do not help much when you are deciding whether to call. So picture an actual week.
Monday, 7:15 a.m. You log in for a fifteen-minute check-in with your peer recovery coach before work. They ask how the weekend went, what you noticed, what you want to track this week. You close the laptop and head into your normal day.
Tuesday, 6:00 to 9:00 p.m. Group therapy. You eat dinner first, then sit down at the kitchen table or in a quiet corner with headphones. There are six to ten other adults on the screen, a licensed counselor running the session, and a topic, relapse triggers, family communication, anger, sleep. You talk. You listen. People you have come to recognize say things that sound exactly like what is happening in your own head.
Thursday, 12:30 p.m. A thirty-minute medication visit with your prescriber over your lunch break. They ask how the buprenorphine or naltrexone is sitting, whether the cravings have softened, whether you are sleeping. They adjust the dose if needed. You eat a sandwich after.
Thursday evening. Another three-hour group, same format, different topic. By week three you stop dreading it.
Saturday, 10:00 a.m. Individual therapy, fifty minutes. The deeper work, the trauma underneath the drinking, the marriage, the grief, the part you do not say in group.
Sunday. No scheduled session. You use the program's mobile tools, message your peer coach if the day gets hard, and reset for the week ahead.
That is roughly nine to twelve clinical hours plus medication management, the same dose of care a traditional IOP delivers, fit around a job and a family. Research on virtual IOP shows attendance and engagement actually run higher than in traditional in-person IOP, and MAT compliance holds up well. The reason is not magic. It is that you do not have to drive an hour each way after work to get there.7
Privacy, Your Job, and Who Has to Know
The honest worry, the one that keeps a lot of people from making the call, is not really about whether the treatment works. It is about whether anyone is going to find out.
Here is what the answer actually looks like.
Your treatment is protected health information. Federal law treats substance use disorder records with an extra layer of confidentiality on top of standard HIPAA, which means a virtual program cannot share that you are a patient with your employer, your spouse, your insurance broker, or anyone else without your written permission. That protection works the same way whether you walk into a clinic or log in from your couch.
What your insurance company sees is a claim, the same kind they see for any other medical visit. They do not send a report to your HR department. Self-pay is also an option if you would rather keep the claim off your insurance entirely.
What your employer sees is whatever you decide to tell them. Most virtual IOP runs in the early morning, the evening, and on weekends precisely so you do not have to explain a string of mid-afternoon absences. If you do need protected time, the Family and Medical Leave Act and the ADA cover treatment for substance use disorders for eligible employees, and you can use them without disclosing a diagnosis to your manager directly, only to HR or a leave administrator.
What the people in your house see is a laptop and a closed door. You are allowed to tell them as much or as little as you want, and a good program will help you figure out what to say to a partner or a teenager when the time feels right. You do not owe anyone the whole story on day one.
When Online Rehab Is the Wrong Call
A guide that only sells you on virtual care is not actually trying to help you. So here is the part most websites skip: when online rehab is not enough, and you should know it before you start.
If you are in active medical danger, virtual care cannot reach you. That includes severe alcohol withdrawal with a history of seizures or delirium tremens, high-dose benzodiazepine withdrawal, an overdose in the last 72 hours, or any withdrawal happening alongside unstable heart, liver, or kidney disease. Those situations need a hospital or a medically managed inpatient detox, not a video visit.
If you are in a psychiatric crisis, including active suicidal intent with a plan, psychosis, or mania, you need an emergency department or a crisis line right now, not an intake form. Pathfinder treats co-occurring anxiety, depression, and trauma alongside substance use, but it is not a primary mental health crisis service and it is not a substitute for one.
If your home is not safe to recover in, where the people you live with are still using around you, where there is violence, or where there is no private corner to take a session, a residential program may be the more honest choice for the first stretch.
And if you have tried outpatient care multiple times and kept relapsing in the first weeks, a higher level of care for a defined period, then a step down to virtual, is often the smarter sequence. The research supports hybrid and stepped care, not virtual-only as a universal answer. A program worth trusting will tell you that on the first call.1
How Pathfinder Delivers Virtual Care in VT, MA, CT, and NH
Pathfinder Recovery is a fully virtual addiction treatment program licensed to serve adults across Vermont, Massachusetts, Connecticut, and New Hampshire. There is no flagship building you drive to. The program is the platform, the clinicians, and the plan that connects them.
The care team includes licensed therapists who run individual and group sessions, prescribers who handle medication for addiction treatment including buprenorphine, naltrexone, and Suboxone, and peer recovery coaches who have walked their own road through substance use disorder. When anxiety, depression, or trauma show up alongside the substance use, that co-occurring care is built into the same program rather than referred out, so you are not retelling your story to three different clinicians. Pathfinder does not provide primary mental health treatment on its own; the mental health work is integrated specifically with substance use disorder care.
The full continuum lives in one place: ambulatory detox support at home, MAT, virtual IOP, individual therapy, group therapy, peer coaching, and family sessions. You access all of it through a secure telehealth platform with a mobile app, which means a session from a hotel room on a work trip looks the same as a session from your kitchen.
What is missing on purpose: waitlists, commutes, and the thirty-day leave of absence. You can start this week, keep your job, sleep in your own bed, and still get the level of care that research recognizes as evidence-based for adults with substance use disorders.4
What to Do This Week If You're Considering It
You do not have to decide everything today. You only have to take the next small step.
If the question that brought you here is still sitting in your chest, try this sequence over the next seven days.
Today. Write down what you have been using, how often, and for how long. Not for anyone else. For the call you are about to make. A clinician will ask, and having it written down means you do not have to find the words while your heart is pounding.
Tomorrow. Make the call or fill out the intake form. A virtual program serving Vermont, Massachusetts, Connecticut, or New Hampshire can usually schedule an assessment within a few days, sometimes the same week. There is no waitlist to clear.
Within the week. Sit through the assessment. Ask about MAT if opioids or alcohol are part of the picture. Ask what the schedule looks like around your job. Ask what happens if you have a hard night.
That is the whole list. You are not committing to thirty days of anything yet. You are finding out what is possible. That is already a step most people never take, and it counts.
Frequently Asked Questions
Can I really go to rehab entirely online, or do I have to show up in person at some point?
You can complete the entire program online if you live in a state where the provider is licensed, including Vermont, Massachusetts, Connecticut, and New Hampshire for Pathfinder. Detox monitoring, MAT prescribing, IOP, individual therapy, and group all happen by video. SAMHSA recognizes telehealth-delivered SUD care as evidence-based practice across that full continuum. Some people choose to add an in-person visit for personal reasons, but it is not required for most adults.4
Can I get medication like buprenorphine through a video visit without an in-person exam first?
Yes. In 2024, SAMHSA made the COVID-era telehealth flexibilities permanent, which means a licensed prescriber can evaluate you and start buprenorphine through a video visit, no initial in-person exam required. Naltrexone has always been simpler to prescribe by telehealth because it is not a controlled substance. The prescription goes to your pharmacy. Follow-up dose adjustments and check-ins continue on the same screen, alongside therapy and peer support.5
Is virtual rehab as effective as going to an in-person program?
The research says yes for most adults. A 2025 meta-analysis found that remote and digital interventions reduced relapse and the number of days people used substances, especially when part of a continuum of care. A VA study showed that giving patients telehealth tablets actually increased the frequency of SUD therapy and group visits rather than letting attendance slip. Hybrid models, where most care is virtual with occasional in-person touchpoints, often perform best.3,9
Will my employer or insurance company find out if I start online rehab?
Your employer will not be told. Substance use disorder records carry an extra layer of federal confidentiality on top of HIPAA, so the program cannot share your status with your employer without your written permission. Your insurance company sees a medical claim, not a report sent to HR. If you want even more distance, self-pay keeps the claim off insurance entirely. What you tell your manager, your spouse, or anyone else stays your decision.
Can I detox safely from home, or do I need to go to a facility?
Many people withdrawing from alcohol or opioids can detox at home with prescription medications and daily video and phone monitoring. A VA study found that low-cost phone monitoring during detox reduced repeat detox episodes. What home detox cannot handle: severe alcohol withdrawal with seizure history, high-dose benzodiazepine withdrawal, unstable medical conditions, or an unsafe home environment. A real intake assessment tells you which category you are in. You do not have to guess.10
How many hours a week does virtual IOP take, and can I keep working?
Virtual IOP typically runs nine to twelve clinical hours a week, usually split across two or three group sessions plus individual therapy and a medication visit. Sessions are scheduled in early mornings, evenings, and weekends so you can keep your job. Research on virtual IOP shows attendance and engagement actually run higher than traditional in-person IOP, and MAT compliance holds up well. Most people work their normal schedule and fit treatment around it.7
No items found.
[{"@context":"https://schema.org","@type":"BlogPosting","headline":"Can I Go to Rehab Online?","description":"Learn how online rehab offers effective medical detox, therapy, and support with licensed clinicians, plus when in-person care is necessary.","publisher":{"@type":"Organization","name":"Pathfinder Recovery"},"mainEntityOfPage":{"@type":"WebPage","@id":"https://www.pathfinder-recovery.com"}},{"@context":"https://schema.org","@type":"FAQPage","mainEntity":[{"@type":"Question","name":"Can I really go to rehab entirely online, or do I have to show up in person at some point?","acceptedAnswer":{"@type":"Answer","text":"You can complete the entire program online if you live in a state where the provider is licensed, including Vermont, Massachusetts, Connecticut, and New Hampshire for Pathfinder. Detox monitoring, MAT prescribing, IOP, individual therapy, and group all happen by video. SAMHSA recognizes telehealth-delivered SUD care as evidence-based practice across that full continuum. Some people choose to add an in-person visit for personal reasons, but it is not required for most adults."}},{"@type":"Question","name":"Can I get medication like buprenorphine through a video visit without an in-person exam first?","acceptedAnswer":{"@type":"Answer","text":"Yes. In 2024, SAMHSA made the COVID-era telehealth flexibilities permanent, which means a licensed prescriber can evaluate you and start buprenorphine through a video visit, no initial in-person exam required. Naltrexone has always been simpler to prescribe by telehealth because it is not a controlled substance. The prescription goes to your pharmacy. Follow-up dose adjustments and check-ins continue on the same screen, alongside therapy and peer support."}},{"@type":"Question","name":"Is virtual rehab as effective as going to an in-person program?","acceptedAnswer":{"@type":"Answer","text":"The research says yes for most adults. A 2025 meta-analysis found that remote and digital interventions reduced relapse and the number of days people used substances, especially when part of a continuum of care. A VA study showed that giving patients telehealth tablets actually increased the frequency of SUD therapy and group visits rather than letting attendance slip. Hybrid models, where most care is virtual with occasional in-person touchpoints, often perform best."}},{"@type":"Question","name":"Will my employer or insurance company find out if I start online rehab?","acceptedAnswer":{"@type":"Answer","text":"Your employer will not be told. Substance use disorder records carry an extra layer of federal confidentiality on top of HIPAA, so the program cannot share your status with your employer without your written permission. Your insurance company sees a medical claim, not a report sent to HR. If you want even more distance, self-pay keeps the claim off insurance entirely. What you tell your manager, your spouse, or anyone else stays your decision."}},{"@type":"Question","name":"Can I detox safely from home, or do I need to go to a facility?","acceptedAnswer":{"@type":"Answer","text":"Many people withdrawing from alcohol or opioids can detox at home with prescription medications and daily video and phone monitoring. A VA study found that low-cost phone monitoring during detox reduced repeat detox episodes. What home detox cannot handle: severe alcohol withdrawal with seizure history, high-dose benzodiazepine withdrawal, unstable medical conditions, or an unsafe home environment. A real intake assessment tells you which category you are in. You do not have to guess."}},{"@type":"Question","name":"How many hours a week does virtual IOP take, and can I keep working?","acceptedAnswer":{"@type":"Answer","text":"Virtual IOP typically runs nine to twelve clinical hours a week, usually split across two or three group sessions plus individual therapy and a medication visit. Sessions are scheduled in early mornings, evenings, and weekends so you can keep your job. Research on virtual IOP shows attendance and engagement actually run higher than traditional in-person IOP, and MAT compliance holds up well. Most people work their normal schedule and fit treatment around it."}}]}]
Pathfinder Recovery offers in-home addiction and mental health treatment that fits your life — not the other way around.From at-home detox and MAT to virtual IOP and peer support, our licensed clinicians bring evidence-based care to you through secure telehealth.
The Pathfinder Recovery App and Smart Ring keep your care team connected to your progress between sessions — monitoring sleep, stress, and recovery milestones in real time.It’s proactive, private, and personalized — so support is always within reach.
Substance Use Recovery with Pathfinder Recovery offers accessible virtual care that supports healing, mental health, and long-term recovery from the comfort of home.
Learn how virtual treatment offers flexible, private support that fits unpredictable work schedules and boosts recovery success with practical strategies.