
MAT With Subutex: What You Need to Know
MAT With Subutex offers compassionate, evidence-based online medication-assisted treatment, supporting safe recovery and long-term substance use care.
November 7, 2025


Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
It's 7:42 PM on a Tuesday. You've answered the last email from a client in a different time zone, the children are finally settled, and the wine bottle in the kitchen is doing what it's done every Tuesday for the past two years. You've thought about getting help. You've also thought about what happens to your bar number, your hospital privileges, your security clearance, your client roster, or your book of business if anyone finds out.
That tension—wanting to stop, refusing to compromise your career to do it—is the actual problem. Not motivation. Not willpower. Logistics, privacy, and a calendar that already runs from 6 AM to 9 PM.
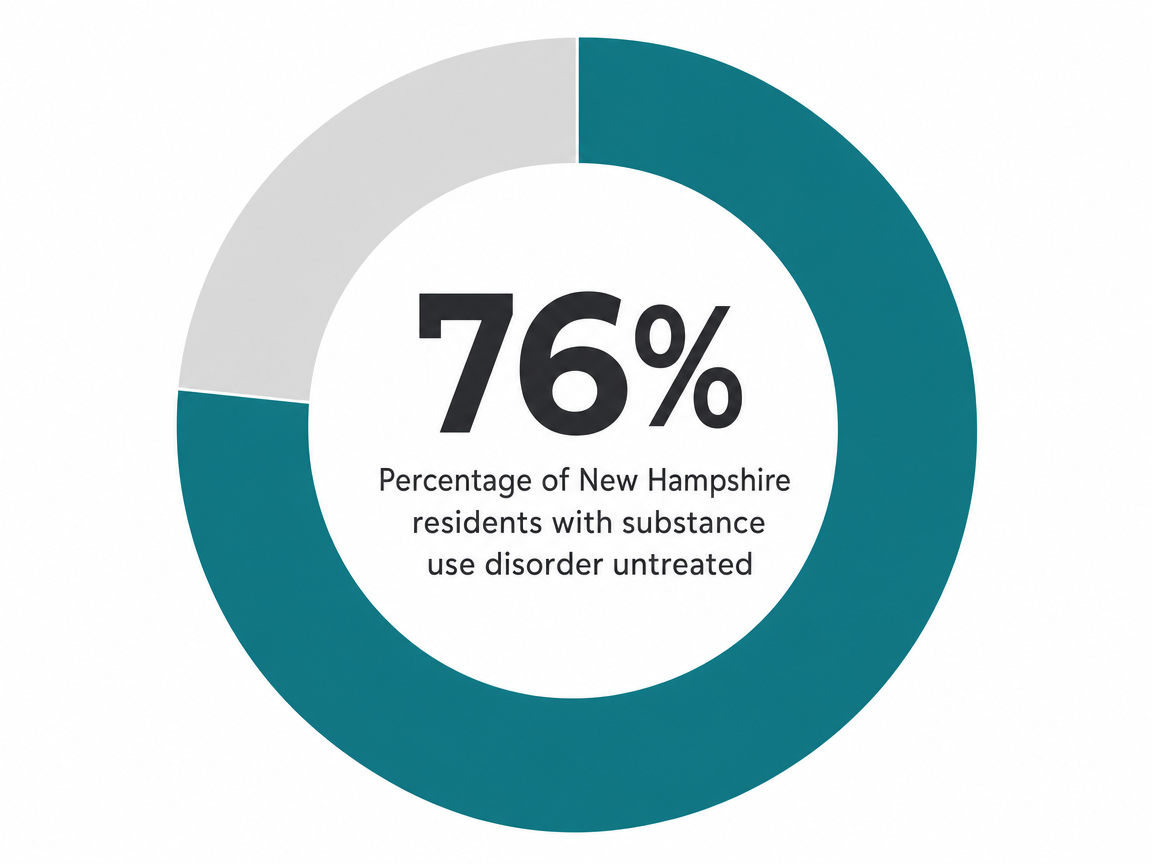
You're not alone in the math, either. In New Hampshire, an estimated 202,000 residents aged 12 and older meet criteria for a substance use disorder, while only about 4.67% receive treatment in a given year, according to SAMHSA's most recent state estimates. Many of those untreated people aren't in denial. They're functional. They're booked. They can't sit in a waiting room three towns over without the receptionist being someone's cousin.10
Virtual holistic treatment is built for this exact bind. Not as a softer version of real care, but as the same evidence-based outpatient model—medication-assisted treatment, therapy, mindfulness-based relapse prevention, peer coaching, body-based practices, co-occurring mental health support—delivered through a screen in the 90-minute window you can actually protect. The rest of this guide walks through what that looks like in NH specifically: what 'holistic' really includes, whether the evidence holds up, how a working week fits, and the questions you probably haven't asked anyone out loud yet.
When clinicians use the word holistic in a real treatment plan, they mean something specific: addressing the substance use, the brain chemistry driving cravings, the trauma or anxiety underneath, the body that's been running on cortisol and bourbon, and the social isolation that keeps the whole loop spinning—at the same time, in one coordinated plan. Not as add-ons. As the plan.
In a virtual program built for working professionals, that integrated plan typically includes seven moving parts:
The reason this bundle matters—rather than picking one piece off the menu—is that the evidence keeps pointing the same direction. A review of yoga and mindfulness interventions integrated into virtual SUD care found the bundled approach reduced relapse risk by roughly 15–25% compared with standard outpatient care alone, though the authors note the field still needs more SUD-specific randomized trials. The signal is real. The footnote is honest.5
What you should hear in that: holistic isn't a softer track for people who want to avoid medication. It's the version where the medication, the therapy, and the body work talk to each other, on one schedule, run by clinicians who share notes. That's the thing worth your Tuesday night.
You bill by the hour. You read studies. You're not going to swap a real treatment plan for a Zoom meditation circle because someone called it 'innovative.' Good. Skepticism here is healthy.
So look at what's actually been measured. A 2025 analysis of how telehealth reshaped SUD care after 2020 found that virtual delivery did not produce worse outcomes than in-person treatment, and patients who accessed care via telehealth showed no increase in adverse events compared with those treated in clinics. That's the floor: virtual is not a downgrade.1
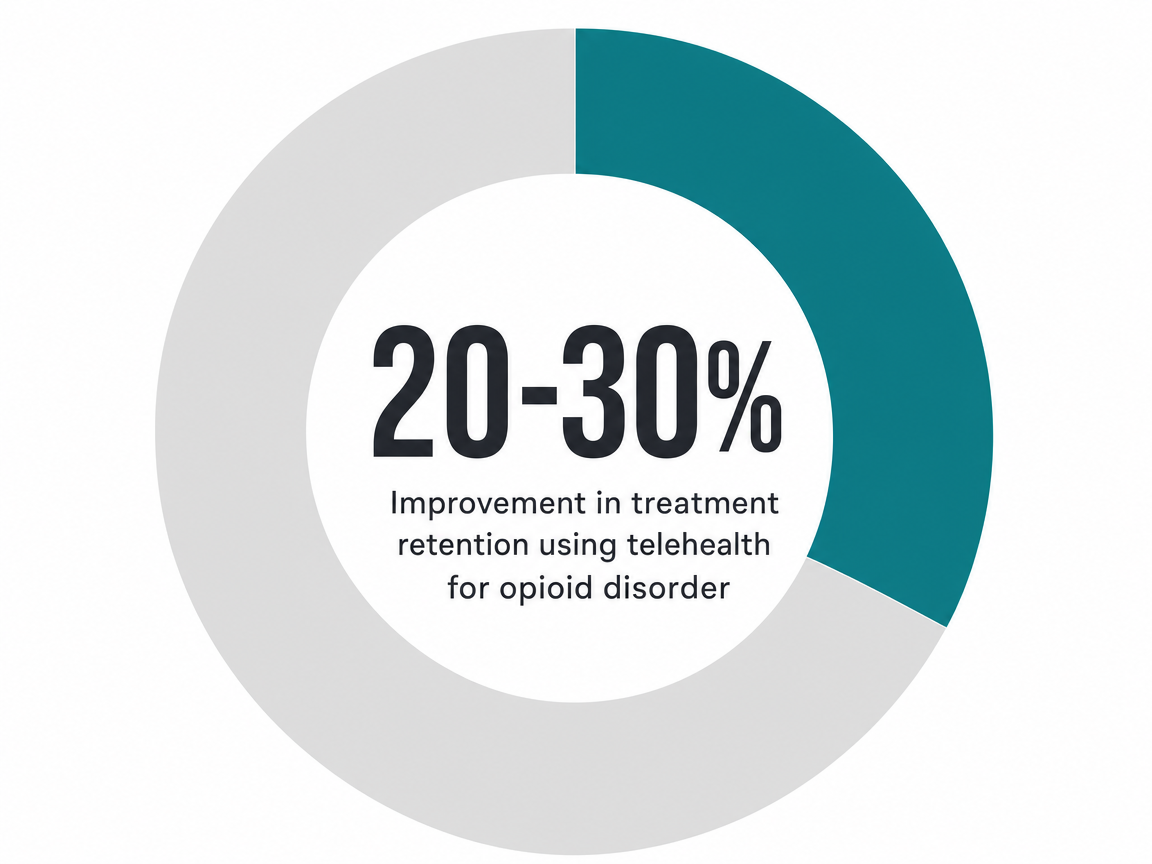
The ceiling is more interesting. For opioid use disorder specifically, telehealth-delivered care in rural areas has been associated with 20–30% improvements in treatment retention—the variable that predicts almost everything else in OUD recovery. Retention matters because the medication only works while you're taking it, and the therapy only works while you're showing up. A modality that gets you to week 12 instead of dropping out at week 4 isn't a soft win. It's the win.4
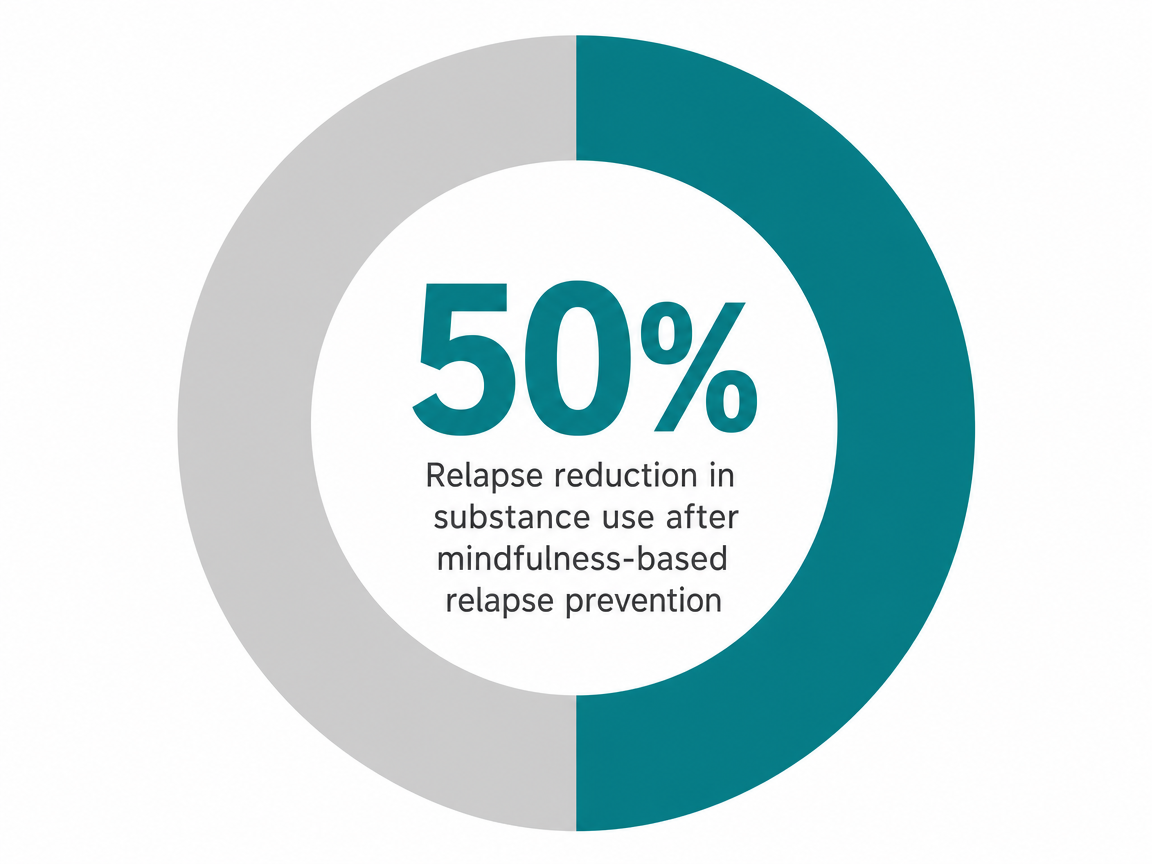
On the holistic side, the evidence is layered. Mindfulness-based relapse prevention (MBRP), the structured 8-week protocol used in many virtual programs, has shown relapse reduction of roughly 50% in some controlled studies, though that figure comes from specific samples and shouldn't be read as a guarantee for every person or substance.7
What this means on a Tuesday night: you're not choosing between rigorous care and convenient care. You're choosing the delivery method that the evidence says will most likely keep you in the chair long enough for the treatment to work.
Pull up a map of New Hampshire and the access problem becomes obvious. Outside the I-93 corridor and a handful of hospital systems, you're looking at counties where the nearest licensed addiction psychiatrist might be a 90-minute drive in good weather. In Coos, Carroll, Sullivan, Grafton—much of the state, really—a 6 PM IOP session in person means leaving the office at 4:30 and getting home at 9:30, three nights a week. That's not a treatment plan. That's a second job you'll quit by week three.
The numbers tell the same story. In SAMHSA's most recent state estimates, roughly 16.57% of New Hampshire residents aged 12 and older meet criteria for a substance use disorder, while only about 4.67% receive any treatment in a given year—leaving nearly 76% of those who need care without it. Some of that gap is stigma. A lot of it is logistics: distance, work hours, child care, and the small-town reality that the parking lot of the only clinic in town is visible from your client's office window.10
Virtual care collapses the geography. A peer-reviewed study of telehealth for opioid use disorder in rural areas found that delivering MAT and counseling through video improved treatment retention by 20–30% compared with in-person-only models—a meaningful gain in exactly the kind of low-density region most of NH qualifies as. Retention is the variable that drives outcomes; if you stay in care, the medication and the therapy get a chance to work.4
Licensure is the other piece working in your favor. Reputable virtual programs serving New Hampshire are staffed by clinicians licensed in NH—and often in Vermont, Massachusetts, and Connecticut as well. If your job has you in a Boston office on Monday, a Burlington client site Wednesday, and home in Nashua by Thursday night, your therapist and prescriber can keep seeing you across state lines because their licensure already covers the region. Your treatment doesn't pause when your calendar moves.
One honest caveat: virtual care is not the right starting point for medically complex withdrawal—severe alcohol or benzodiazepine dependence, for example, where seizure risk is real. Those situations need supervised stabilization first. For most working professionals dealing with alcohol, opioids, or stimulants, though, the geography problem is the actual barrier, and a screen is the thing that removes it.
Here's the part most articles skip: what does this actually look like Monday through Sunday, when you have depositions, a board meeting, a child's hockey practice, and a 7 AM standup with a team in Dublin?
A standard virtual intensive outpatient program in New Hampshire runs about 9 hours of clinical time per week, usually structured as three group sessions of three hours each. Add a 50-minute individual therapy session, a 20-minute MAT check-in with the prescribing clinician (less frequent once you're stable), and a 30-minute peer coaching call. That's roughly 11 hours of treatment, which sounds like a lot until you realize most of it lands in the windows you weren't billing in anyway.
A working version of the week often looks like this:
Most virtual programs let you flex within those slots—if a Wednesday group conflicts with a non-negotiable trial prep, you can sometimes attend a make-up cohort earlier or later in the week. Recordings of psychoeducational content are often available; live group attendance is not optional, because the group is the treatment.
Two things to know about the medication side. First, MAT prescribing happens entirely over video in NH; e-prescriptions go to your usual pharmacy, no separate clinic visit required. Second, retention is what makes this whole structure work. Telehealth-delivered MAT in rural areas has been associated with 20–30% better treatment retention than in-person-only models, which is the reason this calendar can survive your actual life. The schedule isn't gentler than residential care. It's just one you can keep showing up to in week 8, week 16, week 32—when the work is finally getting done.4
If you rolled your eyes at the word yoga three sections ago, that's fair. The recovery industry has earned that eye-roll with a decade of pastel marketing and vague promises about 'healing.' So let's set the soft language aside and look at why a careful clinician puts these practices in your treatment plan anyway.
Start with mindfulness-based relapse prevention. MBRP isn't ambient meditation—it's a structured, manualized 8-week protocol that trains you to notice a craving the moment it shows up, watch it without reacting, and let it pass before it becomes a 9 PM trip to the liquor store. In controlled studies, MBRP has been associated with relapse reduction of roughly 50% in the specific samples studied, with the caveat that those samples weren't infinite and the effect won't be identical for every person or every substance. The mechanism isn't mystical. You're rebuilding the gap between trigger and behavior, which is exactly what your prefrontal cortex stopped doing reliably somewhere around year three of heavy use.7
Yoga and breathwork earn their spot for a different reason. The VA Whole Health Library, reviewing complementary approaches to SUD, reports that yoga is associated with improved treatment retention and that acupuncture has shown reductions in withdrawal symptoms—both with the honest note that high-quality randomized trials are still limited. Retention again. The same variable that drives every outcome that matters.6
Delivered virtually, these aren't performance pieces. A live trauma-informed yoga session over video is 30 minutes in your living room with the camera angled at the ceiling if you want. A breathwork practice is four minutes between meetings. The point isn't transcendence. The point is that your body has been in fight-or-flight for a long time, and giving it a way to downshift makes the rest of the treatment plan—the medication, the therapy, the group—work better.
Here's the part most working professionals figure out alone: the drinking or the pills aren't really about the drinking or the pills. They're about the 2 AM rumination after a hard ruling, the pre-meeting dread that's been there since residency, the low hum of depression you've been outrunning with productivity for fifteen years. Treat the substance and ignore the rest, and you've handed yourself a relapse waiting for its moment.
A virtual program built for this reader treats co-occurring anxiety and depression alongside the SUD, in the same plan, with clinicians who share notes. That means your therapist isn't doing CBT for alcohol use on Tuesday while a separate provider you'll never schedule handles the panic attacks. The psychiatrist managing your MAT is the same person evaluating whether an SSRI or a non-stimulant anxiolytic belongs in the picture. The MBRP work you're already doing in group does double duty—it reduces relapse risk and quiets the anxiety loop that drives a lot of the use in the first place.7
Two honest notes. Virtual programs in this category treat co-occurring conditions as part of SUD care, not primary mental health treatment for someone without a substance use disorder. And if your depression includes active suicidality or your anxiety has tipped into something a higher level of care should hold, a good clinician will tell you that on the intake call rather than enroll you anyway. Integrated treatment is the standard. Honesty about its limits is part of why it works.
You haven't asked anyone these questions because asking them in the wrong room is the problem. So here are the answers, in plain language.
Will my licensing board find out? No, not from a clinician treating you. Your therapist, prescriber, and peer coach are bound by HIPAA and 42 CFR Part 2, the federal rule that gives SUD treatment records an extra layer of protection beyond standard medical privacy. Records can't be released without your written, specific consent—not to your employer, not to your bar association, not to the medical board, not to your spouse. The narrow exceptions involve imminent harm, court orders, or a few mandated reporting situations a clinician will explain on intake. Self-reporting obligations to a licensing board are a separate question with its own rules, and most professional monitoring programs actually view voluntary, evidence-based treatment as a protective factor rather than a red flag.
Will MAT show up on a lab panel or pre-employment screen? Standard workplace drug panels don't typically test for buprenorphine or naltrexone, but specialized panels can. If you have a prescription, you're protected under the ADA in most employment contexts. Talk to your prescriber before any anticipated test so the documentation is in order.
What about EAPs? Employee Assistance Programs can be useful, but the moment you use one, your employer's HR vendor knows you used it—not the diagnosis, but the fact of utilization. Many professionals pay out of pocket or run claims through commercial insurance directly to keep treatment off any employer-adjacent system. That's a legitimate choice, not paranoia.
Can my colleagues see me on a group call? First names only is the norm in virtual IOP. You can use a neutral background, angle the camera, and join from a closed room. Group members sign confidentiality agreements. The trade-off worth naming honestly: cameras-on group is part of how the treatment works, and the discomfort of week one usually fades by week three. That doesn't make it nothing. It makes it survivable, and worth the result.
Two costs matter here: what your insurance covers and what your week can spend. Most commercial PPOs in New Hampshire—Anthem, Cigna, Harvard Pilgrim, Aetna—cover virtual IOP, individual therapy, MAT prescribing, and psychiatric evaluation under behavioral health benefits. Federal parity rules require that SUD coverage match medical-surgical benefits in scope. NH Medicaid covers telehealth-delivered SUD services, including MAT. Self-pay options exist, and a sliding scale is worth asking about directly.
The time cost is the one you'll actually feel. A virtual IOP runs about 9 hours of group plus 1–2 hours of individual and medication contact per week, usually 8–12 weeks before stepping down to weekly outpatient. PHP, a higher level of care, runs 20+ hours per week and is closer to a part-time job. Most working professionals start at IOP unless a clinician's assessment says otherwise.
Before you enroll, ask five questions:
If the answers are specific, the program is built for someone like you. If they're vague, keep looking. You've already done the hard part by reading this far.
The short answer: yes, for most outpatient cases. A 2025 analysis of telehealth SUD care found virtual delivery did not produce worse outcomes than in-person treatment, with no increase in adverse events. The honest caveat: virtual care isn't appropriate for medically complex withdrawal that needs supervised stabilization. For working professionals managing alcohol, opioids, or stimulants at the outpatient level, the evidence says you're not trading rigor for convenience.1
Yes. A psychiatrist or addiction medicine physician can evaluate you over video, prescribe Suboxone, buprenorphine, or naltrexone, and send the e-prescription to your local pharmacy. Follow-up check-ins happen over video too, often in 20-minute windows you can fit into a lunch break. Telehealth-delivered MAT in rural areas has been linked to 20–30% better treatment retention than in-person-only models —the variable that drives almost every outcome that matters.4
Not from a clinician treating you. SUD records get an extra layer of federal protection beyond standard HIPAA, and they can't be released without your specific written consent—not to employers, not to bar associations, not to medical boards. Self-reporting obligations to a licensing board are a separate question with their own rules, and most professional monitoring programs view voluntary, evidence-based treatment as a protective factor, not a red flag.
Plan for about 11 hours of clinical time: three group sessions of three hours each (often 6–9 PM on weeknights), one 50-minute individual therapy slot, a 20-minute MAT check-in, and a 30-minute peer coaching call. Add an optional 30-minute yoga or breathwork session on the weekend. Most programs let you flex within those slots when a deposition or board meeting collides with group, but live group attendance isn't optional—it's where the work happens.
Most commercial PPOs in NH—Anthem, Cigna, Harvard Pilgrim, Aetna—cover virtual IOP, individual therapy, MAT prescribing, and psychiatric evaluation under behavioral health benefits. Federal parity rules require SUD coverage to match medical-surgical benefits in scope. NH Medicaid covers telehealth-delivered SUD services, including MAT. Self-pay and sliding-scale options exist; ask directly. Coverage for adjunct holistic pieces like yoga or acupuncture varies, but the clinical core is typically covered.
Yes, if your clinicians are licensed in each state you work from. Reputable virtual programs serving New Hampshire commonly hold licensure across NH, Vermont, Massachusetts, and Connecticut, which means a Boston Monday, a Burlington Wednesday, and a Nashua Thursday don't interrupt your treatment. Confirm this on intake by asking directly which states your therapist and prescriber are licensed in. If the answer is specific, you're covered. If it's vague, keep asking.
November 7, 2025

November 6, 2025

January 30, 2026