
Virtual Group Therapy in MA: A Complete Guide
Learn how to access quality group therapy virtual MA programs that meet legal standards, ensure privacy, and fit your schedule for effective care.
June 1, 2026


Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
You already know your calendar. Client calls stacked on Tuesdays. A standing leadership meeting that nobody moves. Court dates, charting deadlines, board prep, a build schedule that slips if you blink. Somewhere inside that grid, you're trying to figure out whether you can get real help for a substance use problem without setting your career on fire.
Here's the honest version: yes, you can. And the evidence is not soft.
Virtual substance use disorder treatment has moved from a pandemic workaround to a permanent, clinically credible option. Telehealth availability across SUD treatment facilities jumped 143% between 2020 and 2021 1, and a longitudinal analysis found telehealth addiction treatment initiation increased roughly five-fold during the pandemic 2. That infrastructure didn't roll back. It's how a meaningful slice of working adults now access care.
What that means for you, practically, is this: a confidential video session at 7:00 a.m. before your first meeting, or 6:30 p.m. after the last one, is no longer an asterisk. It's the model. You can sit in your home office, close the door, and meet with a licensed clinician or a peer coach without driving to a clinic, signing in at a front desk, or losing a half-day of billable time.
This article is written for you—someone in Vermont, Massachusetts, Connecticut, or New Hampshire who is quietly weighing whether telehealth care is strong enough to trust with both your recovery and your livelihood. Short answer: it can be. Let's walk through why, and how to actually make it work.
Most articles about treatment treat your job as the obstacle. Something to schedule around, hide from, or eventually take leave from. That framing misses what the research actually shows: for working adults, your career and your recovery are not in competition. They prop each other up.
Start with retention, because retention is where outcomes live. Staying in SUD treatment for at least 90 days is associated with a higher likelihood of employment and earnings down the line 3. The longer you stay engaged, the more your work life stabilizes. That part you might expect.
Here's the part that surprises people: the reverse is also true. A 2023 analysis of telehealth SUD care found that being unemployed raised the risk of dropping out of treatment, with a hazard ratio of 1.37 7. In plain terms, people without a job were significantly more likely to leave care early. Employment isn't just something recovery eventually rebuilds. It's a stabilizer that helps you stay in treatment in the first place.
Your standing 9:00 a.m., your team you don't want to let down, the routine of getting dressed and showing up—those are not obstacles to recovery. They're scaffolding. Structure, purpose, and identity all do clinical work, even on the days you'd rather be doing anything else.
If you're going to bet your career on a treatment model, you want to know it holds up. Fair. The hardest test in addiction medicine isn't whether someone shows up on day one—it's whether they're still in care a year later. That's where the modality earns or loses the argument.
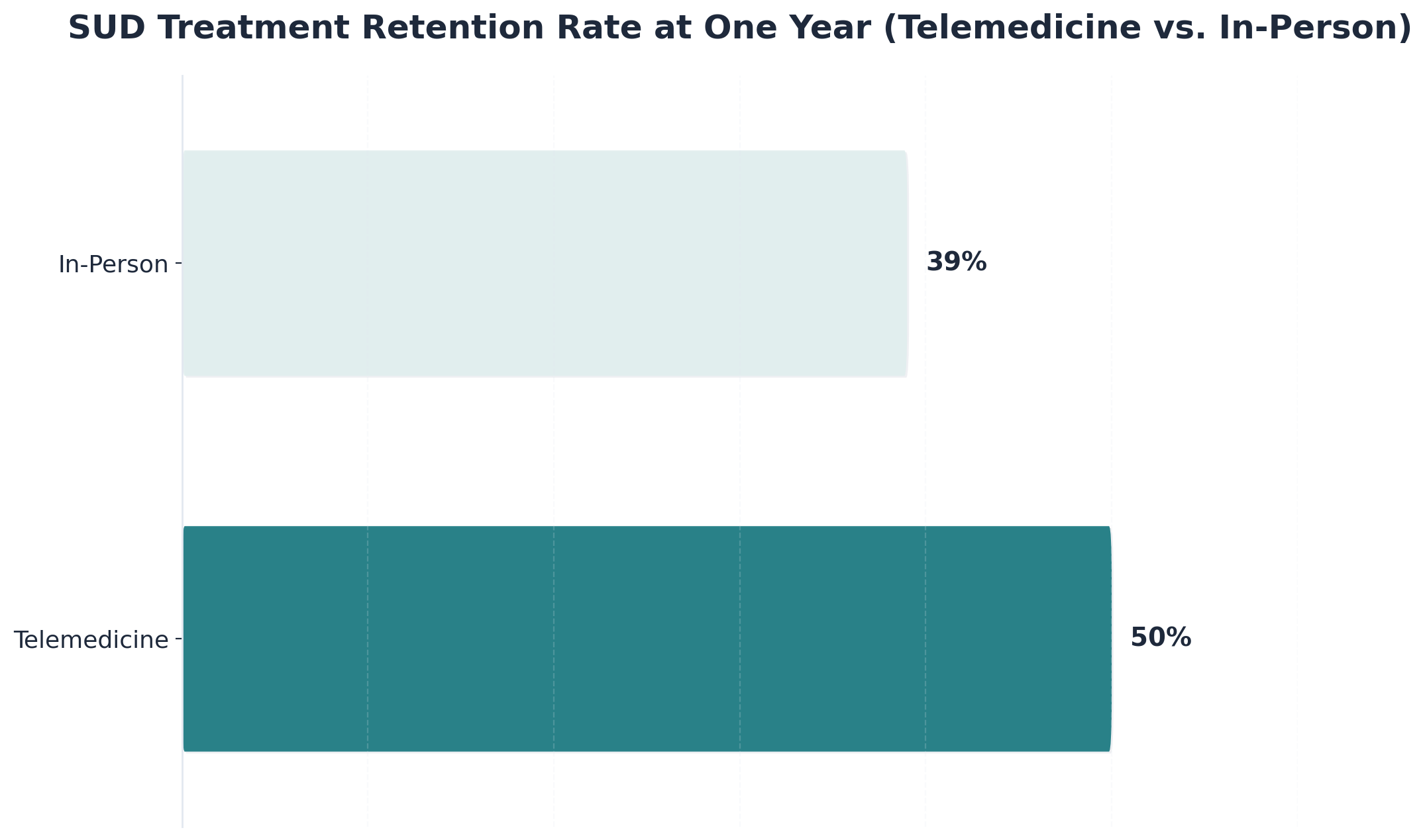
A 2023 review of telepsychiatry for addiction patients found that one-year retention was 50% for telemedicine-delivered SUD care, compared with 39% for in-person treatment 4. The patients studied were adults receiving addiction treatment through licensed clinicians; the comparison was head-to-head against traditional outpatient care. Telemedicine didn't just match the in-person model. It kept more people engaged at the twelve-month mark.
Why does that matter for you specifically? Because retention is the engine. Staying in SUD treatment for at least 90 days correlates with stronger employment and earnings outcomes 3, and a separate 2023 study reported a 12-month retention rate of 81% in a structured outpatient cohort 9—a reminder that when programs are designed well, sustained engagement is achievable, not aspirational.
The mechanism here is not mysterious. When the session moves to your laptop, the friction drops. No commute, no waiting room, no asking your assistant to block off three hours. You log on, do the work, and get back to your life. That's how a 7:00 a.m. appointment in week one becomes a 7:00 a.m. appointment in month eleven.
Staying in care matters. But you also want to know whether people actually get better. The retention number tells you the door stays open; the outcome numbers tell you what happens once you walk through it.
A 2018 Yale study tested a web-based program called CBT4CBT against standard counseling for adults with substance use disorders. Among participants who completed the program, 67% no longer met criteria for substance abuse, compared with 43% of those receiving traditional counseling alone 8. That's a 24-point gap in a randomized comparison. Worth being precise about the scope: this was a specific computerized cognitive behavioral therapy module, studied in a defined adult population, not a blanket claim that every virtual program beats every in-person one. But the direction matters. A well-designed virtual modality can produce better outcomes than what many people picture as the gold standard.
The broader literature backs the pattern up. A 2024 review of telemedicine-delivered SUD treatment concluded that virtual care is generally perceived as beneficial, acceptable, and as effective as in-person care 16. And a 2025 analysis found that clinicians who used telehealth most heavily had lower SUD-related hospitalization rates among their patients 12—a downstream signal that virtual engagement is doing real clinical work.
So yes, this is real medicine. The screen is not the limit. The work you do on either side of it is.
A few years ago, getting SUD care while holding down a demanding job meant taking PTO, driving to a clinic, and sitting in a waiting room where you might run into someone you knew. The geography of treatment was its own barrier. That world is largely gone, and the change is structural, not seasonal.
Two numbers tell the story together. Telehealth availability across SUD treatment facilities rose 143% between 2020 and 2021 1. Over the same stretch, telehealth initiation for addiction treatment grew roughly five-fold during the pandemic, climbing from a small pre-pandemic baseline into a routine entry point for care 2. The first number is the supply side: clinics built the infrastructure. The second is the demand side: people actually used it. When supply and demand both shift that hard in the same direction, the result tends to stay.
And it has stayed. In January 2024, SAMHSA finalized a rule making several telehealth flexibilities permanent for opioid use disorder treatment, including the ability to start buprenorphine through a telehealth visit without a prior in-person evaluation 11. That rule is the regulatory floor under everything you're considering. It means a discreet first appointment from your home office isn't a temporary accommodation a clinic might pull back next quarter. It's policy.
Practically, this changes what's available to you in Vermont, Massachusetts, Connecticut, and New Hampshire. You can be assessed, prescribed appropriate medication, and matched with a therapist and peer coach without ever scheduling a daytime drive. Video, the research shows, is now the preferred channel for most SUD services—chosen over telephone for the bulk of clinical contacts because it preserves more of what makes therapy work 14.
The point isn't that virtual care is new. It's that the access landscape underneath it is now durable. You're not improvising. You're using a system that's been built, tested, and codified into permanent rules.
Treatment doesn't fail working professionals because the clinical model is wrong. It fails because the calendar isn't designed for it. If you book recovery into the leftover gaps of your week, recovery will lose every fight with a Monday escalation. So the work, before the first session, is structural.
Start with the anchors. A typical virtual intensive outpatient program runs three sessions a week, often two to three hours each. Add an individual therapy hour and a peer coaching check-in, and you're looking at roughly nine to twelve hours of clinical contact in week one. That's real time. It's also less than the time most professionals already lose to a long commute or one bad meeting block.
Place the heaviest sessions where your job pulls least. For a lot of people in VT, MA, CT, and NH, that's early morning before the inbox opens, or evening after 6:00 p.m. Video is the format you want here—research on SUD telehealth services found video was chosen over phone for the majority of clinical contacts because it preserves the therapeutic relationship better than a voice call 14. Treat your camera-on session as a real appointment, not a multitask window.
Three rules that hold up under pressure:
Then there's the question of what to call it. The calendar entry on a shared work system does not need to say "therapy." "Personal appointment" or a recurring "hold" is accurate, professional, and yours to keep private. The CDC's workplace recovery guidance is clear that supporting employees in recovery starts with reducing disclosure pressure, not adding to it 13.
The goal isn't a perfect week. It's a week where missing a session feels harder than keeping it.
Not all virtual care is the same dose. Picking the right level is the difference between a plan that holds and one that quietly collapses around month two. Three options are worth knowing by name.
How do you choose? Be honest about two things: how much structure you actually need this month, and how much your week can hold without breaking. A virtual IOP at 6:00 p.m. three nights a week is doable for a lot of professionals, but only if you protect the slot the way you'd protect a board meeting. The 2024 telehealth qualitative work on opioid treatment found that flexibility in follow-up is one of the strongest reasons people stay in care 6—a hint that hybrid approaches, mixing virtual sessions with the occasional in-person touchpoint, work well for some.
If you're unsure, start higher and step down. It's easier to graduate from IOP to outpatient than to climb back up after a slip.
This is the part most working professionals lose sleep over. Not the clinical work itself—the question of who has a right to know you're doing it.
Start with the default: in most cases, no one at your job needs to be told. Treatment is protected health information. A virtual session you take from your home office, on your own time, is not a workplace event. The CDC's NIOSH guidance on workplace-supported recovery is direct that good employer practice means reducing disclosure pressure, not engineering it 13. The Department of Labor's Recovery-Ready Workplace resources point in the same direction—employers are encouraged to build environments where people in recovery can stay employed without having to announce it 15. You can use those frameworks as a tailwind, not a requirement to come forward.
Where it gets more textured is licensure. If you hold a clinical license, a bar membership, a CDL, a contractor's license, or a credential governed by a state board, the rules vary. Some boards have mandatory self-reporting tied to specific events—an arrest, an impairment incident, a formal diagnosis attached to certain disciplinary triggers. Many do not require self-reporting for someone proactively seeking outpatient care that is not impairing their work. The honest answer: you need to read your specific board's language in Vermont, Massachusetts, Connecticut, or New Hampshire, and most boards have a confidential professional health program designed exactly for this situation. Those programs are usually separate from disciplinary tracks and built to keep your license intact while you get care.
If you are considering FMLA, ADA accommodation, or short-term disability, that is a different conversation—those routes do involve HR, and they exist for a reason. For most readers, though, virtual outpatient care simply doesn't trigger them. You're working a normal week and seeing a clinician on Tuesday at 7:00 p.m.
Two principles worth holding onto. First, disclosure is a decision, not a reflex; you can make it later, narrowly, or never, depending on what your situation actually requires. Second, the people you do tell should be chosen for what they can offer—a spouse, a trusted friend, a sponsor, a therapist—not because guilt is asking you to confess. Recovery is yours. So is the story of it.
Virtual care is strong. It's not magic. If you're going to trust this model with your recovery, you should know where it strains.
The first tradeoff is isolation. A video session ends and you close the laptop, and the room is just your room again. There's no parking-lot conversation with someone from group, no five-minute walk to the car where the day decompresses. For some people, that's a feature. For others, it leaves recovery feeling thinner than it should. The fix isn't complicated, but it has to be deliberate: a peer coach you actually call between sessions, an in-person mutual aid meeting once a week, a sponsor whose number you use. A 2024 qualitative study on telehealth for opioid treatment found that flexibility helped retention, but participants often preferred hybrid models that mixed virtual sessions with occasional in-person contact 6. Don't assume fully virtual will be enough on its own. Plan for the human edges.
The second tradeoff is structure. Virtual care is easier to skip. The same low friction that lets you join from your home office also lets you cancel from your home office at 6:55 p.m. because the day was long. The data on dropout deserves a second look here: unemployment raised the dropout hazard 1.37 times in telehealth SUD treatment 7, partly because employment provides the daily structure that keeps appointments from drifting. If you're working, that structure is already on your side. If your job situation shifts mid-treatment, tell your clinician early and add scaffolding before the calendar starts slipping.
The third tradeoff is fit. Some clinical situations—severe withdrawal risk, unstable housing, active suicidality, prior treatment failures—still call for higher-acuity or in-person care. Virtual is the right starting point for many working professionals. It is not the right starting point for everyone, and an honest intake assessment will tell you which one you are.
People talk about what recovery costs—the time, the focus, the energy you're already short on. Less often do they talk about what it gives back. And for working professionals, the give-back side of the ledger is where the real argument lives.
Start with the obvious: substance use, left untreated, taxes the same cognitive resources your job depends on. Sleep gets unreliable. Mornings get heavier. The small slips—a missed detail in a contract, a meeting you didn't quite track—compound. Recovery doesn't make you a different person. It returns the person you already are to the desk.
The employment data tracks this directly. In a year-long SUD intervention study, 59% of participants obtained employment over the course of treatment, with an average time-to-employment of about 17 weeks 10. Worth being clear on scope: that study used an abstinence-contingent wage component and measured people who weren't working at intake, so the headline number isn't a forecast for someone already employed. But the underlying signal holds. As treatment engagement deepens, work outcomes improve.
For you, already employed, the return looks more like compounding than recovery from a low. A clearer head in the Wednesday strategy meeting. A real evening with your family instead of a foggy one. Ninety days of consistent care, the marker associated with stronger employment outcomes 3, starts to feel less like a finish line and more like a floor you're now standing on.
That's the loop. Care steadies the work. The work steadies the care. You get both back.
You've read enough. The question now is what you do tonight, not what you understand in theory.
Pick a 30-minute window this week—after dinner, before bed, the quiet hour you usually scroll through email instead of using. In that window, do three things:
That's the entire next step. You're not signing up for a year. You're getting assessed, hearing what level of care a clinician thinks fits, and learning what your insurance covers. If virtual outpatient or IOP is the right starting point, you can begin within days—no waitlist, no commute, no PTO request. Pathfinder Recovery is one option built specifically for working adults in Vermont, Massachusetts, Connecticut, and New Hampshire, and there are others. The point is to make the call.
Your career and your recovery are not opposing forces. Tonight is a good night to stop treating them like they are.
For most working professionals, yes. Virtual outpatient and IOP sessions are designed to fit early mornings, evenings, and lunch hours, so you can keep your normal schedule. You don't have to file PTO or explain a half-day absence. The pandemic-era growth in telehealth SUD services—up 143% across facilities between 2020 and 2021 1—was built around exactly this kind of access.
Not by default. Treatment is protected health information, and a session you take from home on your own time is not a workplace event. CDC NIOSH guidance encourages employers to support recovery without forcing disclosure 13. Unless you choose to use FMLA, ADA accommodations, or short-term disability, your employer has no automatic visibility into outpatient care. Disclosure is your decision, made on your timeline.
Virtual care handles a wider range of severity than people assume. A 2024 review found telemedicine for SUD is generally as effective as in-person treatment 16. That said, severe withdrawal risk, unstable housing, or active suicidality usually call for higher-acuity or in-person care. An honest intake assessment will tell you which level fits. Starting with a virtual evaluation costs you nothing but a phone call.
Often, yes. SAMHSA's January 2024 final rule made several telehealth flexibilities permanent for opioid use disorder treatment, including starting buprenorphine through a telehealth visit without a prior in-person evaluation 11. Naltrexone for alcohol or opioid use disorder is also commonly prescribed through telehealth. Methadone has more specific rules tied to opioid treatment programs. A licensed clinician in your state can confirm what applies to your situation.
For most boards, voluntarily seeking outpatient care that doesn't impair your work does not trigger mandatory self-reporting. Rules vary by profession and state, so read your specific board's language in VT, MA, CT, or NH. Most states also run confidential professional health programs separate from disciplinary tracks, designed to keep licenses intact while members get care. Talking to a licensure attorney before you disclose anything is a reasonable step.
The core clinical model is the same: video-based individual therapy, group sessions, peer coaching, and medication management with a clinician licensed in your state. What varies is insurance coverage, specific medication policies, and which providers hold licensure where. A provider serving all four states can treat you whether you're in Burlington, Boston, Hartford, or Manchester—as long as you're physically located in a state where your clinician is licensed during each session.
June 1, 2026

November 6, 2025

November 7, 2025