Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
Key Takeaways
New Hampshire administrative code sets a clear line: standard outpatient care runs less than 9 hours per week, while IOP requires 9 or more hours plus five named clinical services including group counseling.1,2
Group therapy is the most commonly used format for substance use disorder treatment in the U.S., and research shows it performs comparably to individual therapy across many conditions.9,11
Access points vary by region and situation: the 10 Community Mental Health Centers cover every county, while hospital programs, private practices, SUD specialty providers, and virtual groups each fit different privacy and scheduling needs.4
Working adults in NH should match format to calendar and intensity, ask programs directly about camera policy and confidentiality, and confirm the provider coordinates MAT and co-occurring mental health care rather than treating groups as the whole plan.1,6
What group therapy actually looks like for a working adult in New Hampshire
Picture a Tuesday evening in Manchester. You've closed your laptop after a long day of meetings, the kids are settled, and at 6:30 p.m. you log into a video call with seven other adults and a licensed clinician. For the next 90 minutes, nobody asks how your quarter went. You talk about cravings, sleep, the wedding coming up where everyone will be drinking, the coworker who keeps offering you a beer after work. That is group therapy, and in New Hampshire it is one of the most common ways adults actually receive care for substance use disorder.
The format is not a watered-down version of one-on-one counseling. New Hampshire's administrative code names individual and group counseling as core required services in both standard outpatient and intensive outpatient programs. A national review of the empirical literature found that group therapy is the most commonly used format for substance use disorder treatment in the United States. You are looking at the mainstream of clinical care, not a side door.1,2,9
What changes for a working adult is logistics. You may not have two hours in the middle of a workday to drive to a clinic in Concord, sit in a waiting room, and drive back. You may not want to. The rest of this guide walks through how outpatient and IOP groups are defined in NH, where they are delivered, how virtual options work, and how to pick a format that fits the week you actually have.
How New Hampshire defines outpatient and intensive outpatient group care
Standard outpatient: less than 9 hours per week
If you have spent any time looking at NH treatment listings, you have probably seen the phrase "outpatient" used so loosely it stops meaning anything. The state actually defines it. Under New Hampshire administrative code, outpatient treatment services for substance use disorder consist of individual or group counseling sessions, or both, totaling less than 9 hours per week. That is the legal ceiling, not a suggestion.2
In practice, this looks like one or two scheduled sessions a week. You might attend a 90-minute group on Wednesday evenings and a 50-minute individual session on Monday morning, and you are still inside the outpatient definition. The rule treats group counseling as a standard, billable service alongside individual counseling, not as a discount substitute.2
For a working adult, standard outpatient is the format that asks the least of your calendar. It assumes you are stable enough to function in your job and home life, and that a few clinical hours a week, paired with sleep, exercise, and whatever else supports you, is enough to keep you moving forward.
Intensive outpatient (IOP): 9 or more hours per week
Cross the 9-hour line and you are in a different regulatory category. Intensive outpatient programs in NH are built for people who need more clinical contact than standard outpatient can offer, but who do not require residential care. The administrative rule requires every licensed IOP to deliver five clinical services:1
screening and assessment
treatment and discharge planning
individual and group counseling
psychoeducational services
crisis intervention
Group counseling is named directly in the rule, not buried in a footnote.
A typical NH IOP runs three sessions per week, three hours each, often in the late afternoon or evening so people can keep working. Most of those hours are group-based. You might spend Monday in a relapse prevention skills group, Wednesday in a process group, and Thursday in psychoeducation on topics like the neurobiology of cravings or repairing trust at home.
IOP is the level of care that most often suits someone in early recovery who is still employed but needs structure beyond a single weekly session, someone stepping down from detox or residential treatment, or someone whose standard outpatient plan has stopped holding.
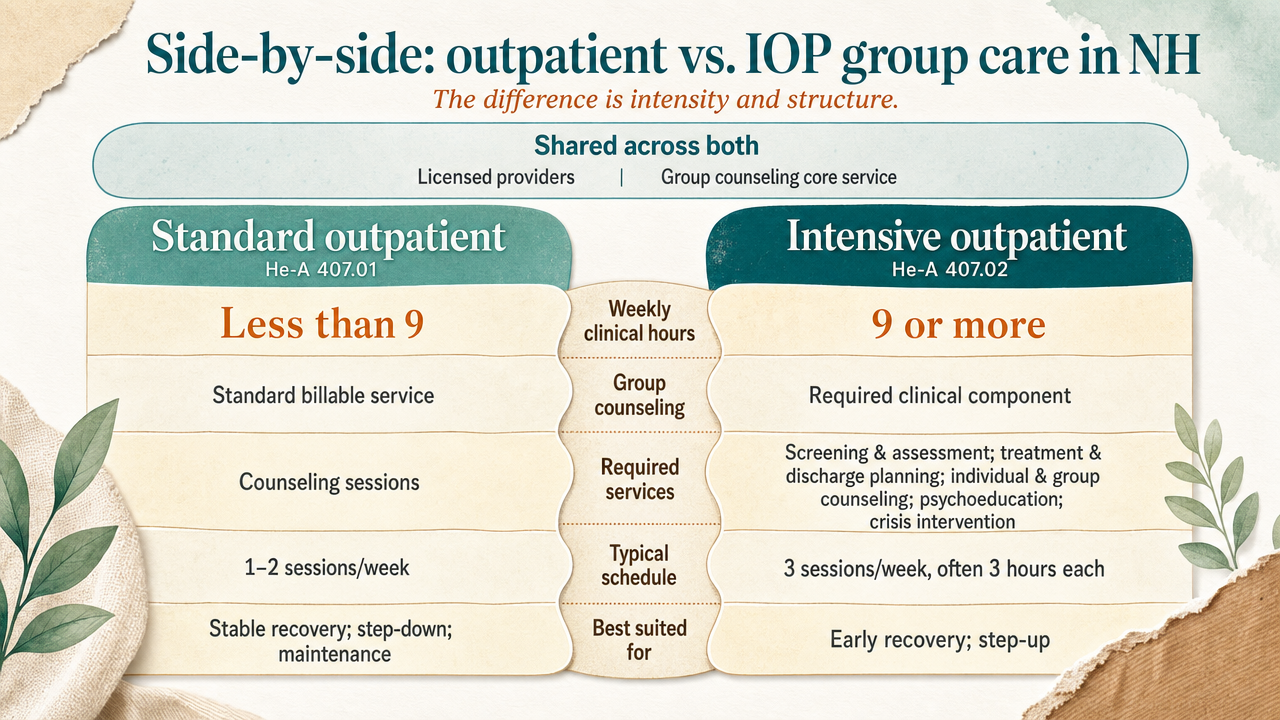
Side-by-side: outpatient vs. IOP group care in NH
The two tiers share more than they differ, which is part of what makes the distinction confusing. Both must be delivered by licensed providers. Both treat group counseling as a core, required service. The split is intensity and structure.
Feature
Standard Outpatient (He-A 407.01)
Intensive Outpatient (He-A 407.02)
Weekly Clinical Hours
Less than 9
9 or more
Group Counseling
Standard billable service, alone or with individual counseling
Required clinical component
Required Services
Counseling sessions
Screening and assessment, treatment and discharge planning, individual and group counseling, psychoeducational services, crisis intervention
Typical Schedule
1–2 sessions per week
3 sessions per week, often 3 hours each
Best Suited For
Stable recovery, step-down, ongoing maintenance
Early recovery, step-down from detox or residential, when standard outpatient is not enough
When you are calling programs in Nashua or Lebanon, the first question to ask is not "do you offer group therapy." It is "are you a 407.01 outpatient program or a 407.02 IOP, and which one fits where I am right now?"
Why group is not a step down from individual therapy
There is a common assumption worth naming directly: that individual therapy is the "real" treatment and group is what you settle for when one-on-one is unavailable or unaffordable. That belief does not match what the evidence shows, and it does not match how SUD care is actually structured in the United States.
A review of the empirical literature on group therapy for substance use disorders concluded that group therapy is the most commonly used format for SUD treatment in the United States. Not a backup. Not a budget option. The primary delivery format. A separate systematic review comparing group and individual psychotherapy in adults across multiple mental health conditions found that, for many disorders studied, group and individual therapy did not differ significantly in effectiveness. That review spans several diagnoses rather than SUD specifically, but it pushes back hard on the reflex that one-on-one is automatically superior.9,11
There is also a scale argument worth taking seriously. According to the National Survey on Drug Use and Health, the percentage of people in the U.S. aged 12 or older with a past-year drug use disorder (self-reported) rose from 8.7% in 2021 to 9.8% in 2024. More adults need care than the system can reach through 50-minute individual sessions alone. Group formats are how the field actually meets that demand at clinical depth, with a licensed clinician guiding the room.5
There is something the group format does that an individual session structurally cannot. When you hear someone two years ahead of you describe the same craving you had on Sunday night, or when a peer pushes back on a story you have been telling yourself about why this time is different, that is clinical work. It is the kind of feedback a therapist, however skilled, cannot manufacture alone in a room with you. For a working professional who has spent years performing competence, sitting in a room with other adults who are not impressed and not fooled is often the part of treatment that finally moves something.
The four group formats you are likely to encounter in a week
Psychoeducational groups: learning the mechanics of recovery
Psychoeducational groups are the format that looks most like a small seminar. A clinician walks the room through a specific topic, and you discuss how it shows up in your own life. The topics are concrete: how alcohol disrupts REM sleep, what fentanyl contamination has done to the drug supply, how cravings actually peak and fall, what your brain is doing in the first 90 days. New Hampshire's IOP rule names psychoeducational services as a required clinical component, so if you enter an IOP in Dover or Keene, you can expect this format on the schedule. The Surgeon General's review treats psychoeducation as a standard, evidence-supported element of SUD care. For a working professional, these groups often feel the safest to start with. You are learning, not confessing.1,6
Skills groups are where you practice. The clinician teaches a specific technique, the group works through it together, and you leave with something to use before the next session. Cognitive behavioral therapy groups have you map the thought that runs from a hard meeting to a drink in your hand, then rehearse interrupting it. Motivational interviewing groups draw out the reasons you actually want change, in your own words, not anyone else's. Relapse prevention groups walk through your high-risk situations—the conference reception, the Sunday afternoon when the house is quiet, the fight with your partner—and build a written plan for each. The Surgeon General's review identifies CBT, motivational interviewing, contingency management, and mutual-help facilitation among the psychosocial approaches with the strongest evidence base for SUD, and notes they are routinely delivered in group format. If you are someone who learns by doing, this is usually the format that clicks first.6
Process groups: working through what is actually happening in your life
Process groups have less structure on the surface and more underneath. There is no slide deck. You bring whatever is loud that week—the family dinner that went sideways, the resentment you have been carrying about your boss, the shame after a near-slip on Friday—and the group, guided by a clinician, helps you look at it. The literature review on SUD group therapy includes process groups among the standard formats used across outpatient, IOP, and residential settings. The work happens through the room, not just from the clinician. Someone reflects back a pattern you could not see. Someone names the thing you were avoiding. For professionals used to staying in control of how they are perceived, process groups are often the hardest to start and the ones that produce the most movement once you stay with them.9
Mutual-help facilitation: bridging clinical care and peer support
Mutual-help facilitation is not the same as attending an AA or SMART Recovery meeting, though it points you toward those. In a facilitated group, a clinician helps you understand how mutual-help communities work, what each tradition actually teaches, and how to use them alongside clinical care. The Surgeon General's review identifies mutual-help group facilitation as an evidence-based component of SUD treatment. For a working adult in NH, this format is practical. Clinical groups happen on a set schedule. Mutual-help meetings, in person across the state or online at almost any hour, give you a place to land between sessions and after your formal program ends.6
Recovery, Made Possible — From Home
Pathfinder Recovery offers in-home addiction and mental health treatment that fits your life — not the other way around. From at-home detox and MAT to virtual IOP and peer support, our licensed clinicians bring evidence-based care to you through secure telehealth.
The 10 Community Mental Health Centers as a public-sector access point
If you are not sure where to start, the Community Mental Health Center system is the most predictable on-ramp in New Hampshire. The state is divided into 10 CMHC regions, each anchored by a designated provider with a main office and satellite locations. Together they cover every county, from the North Country down through the Lakes Region, the Upper Valley, the Monadnock area, the Seacoast, and the Merrimack Valley.
The service array is consistent across regions. Each CMHC offers 24-hour emergency services, assessment and evaluation, individual and group therapy, case management, community-based rehabilitation, psychiatric services, and community disaster mental health support. Group therapy is not an add-on at these centers. It is part of the standard offering you can ask about by name when you call.4
For a working professional, the CMHC route has trade-offs. You can usually access care regardless of insurance status, which matters if you are between jobs or on a high-deductible plan. The center handles the coordination if you also need psychiatric medication or case management. The honest limit is that CMHCs primarily organize around serious mental illness and crisis care, so SUD-focused group options vary by region and may have wait times. Call the CMHC for your county first and ask specifically which groups are running this month and who they are designed for.
Hospital programs, private outpatient practices, and SUD-specialty providers
Outside the CMHC network, you have three other places to look. NH hospital systems run behavioral health outpatient programs, often with structured IOP tracks that include group counseling as a required component under state rule. These programs tend to be well-staffed and tightly coordinated with medical care, which matters if you are managing withdrawal, chronic pain, or psychiatric medication alongside SUD work.1
Private outpatient practices are the second category. Many licensed clinicians and small group practices run weekly therapy groups under the standard outpatient definition of less than 9 hours per week of counseling. Groups at this level are often topic-focused: early recovery, women's groups, professionals' groups, family members.2
SUD-specialty providers are the third. These programs are built specifically around addiction care and typically run the full ladder, from standard outpatient through IOP and partial hospitalization, with group counseling as the spine of the schedule. The Surgeon General's review treats this kind of structured outpatient and IOP delivery as a core part of evidence-based SUD care. If you already know SUD is the primary issue, a specialty provider usually offers the most concentrated group experience.6
Virtual groups for VT, MA, CT, and NH residents
Virtual delivery is what has actually changed the math for working professionals in New Hampshire. A group that meets at 6 p.m. on Tuesday no longer requires you to leave the office by 4:30 to make it through Manchester traffic to a clinic in Concord. You close one tab and open another. For people in the North Country, where the nearest specialty SUD provider might be an hour each way, virtual access is sometimes the only realistic option for sustained IOP-level group work.
NH's regulatory definitions do not change when care moves to video. A virtual IOP still has to meet the 9-or-more-hours-per-week threshold and deliver the five required clinical services, including group counseling. A virtual standard outpatient group still falls under the less-than-9-hours rule. The licensure, documentation, and clinical structure are the same. What changes is the room.1,2
Several providers now deliver virtual group therapy specifically for adults living in Vermont, Massachusetts, Connecticut, and New Hampshire, with clinicians licensed in each state. If you live near a state line, work across one, or travel for your job within the four-state region, that footprint matters. It also means your group is more likely to include people whose daily life looks like yours, not just people from your zip code.
Discretion, privacy, and the camera-on question
New Hampshire is a small state. The person across from you in a Concord waiting room might be a client, a neighbor, or the parent of your kid's soccer teammate. That is a real consideration for working professionals, not a vanity concern, and good programs treat it as a clinical variable rather than a marketing line.
Start with the legal floor. Every licensed group, in person or virtual, operates under confidentiality rules that bind both the clinician and the participants. In an opening session, the facilitator typically walks the group through what stays in the room: names, stories, employer details, anything identifying. Breaking that agreement is grounds for being removed from the group.
Virtual groups add a layer most readers do not anticipate until they are in one. You control your environment. You can attend from a locked home office, a parked car between meetings, or a quiet corner of a hotel room when you are traveling for work. Nobody at the office sees you walk into a building with a clinical logo on the door. For people in roles where being recognized at a treatment center would be professionally costly, that single shift changes whether care happens at all.
The camera-on question is worth asking directly when you screen a program. Most clinical groups expect cameras on during session, because facial cues and presence are part of how the work happens. Reputable virtual providers will explain their policy upfront, describe how they handle screen names, and tell you who can see the participant grid. If a program will not give you a clear answer on those three points, keep calling.
When group alone is not enough: co-occurring needs and MAT
Group therapy is powerful, and it has limits. About 4% of New Hampshire's population lives with a serious mental illness like schizophrenia, bipolar disorder, or major depression, and many people in SUD treatment carry a co-occurring condition that needs its own clinical attention. A skills group on relapse prevention will not, on its own, manage untreated depression or stabilize a mood disorder. You need both threads worked at once.12
The NH IOP rule already assumes this. It requires screening and assessment, treatment planning, and crisis intervention alongside group counseling, which means a competent program is looking for what else is happening, not just counting your group hours. If you are dealing with SUD and a co-occurring mental health condition, integrated care that addresses both together is the standard, not a referral somewhere else next month.1
Medication-assisted treatment is the other piece. For opioid or alcohol use disorder, medications like buprenorphine, naltrexone, or methadone are evidence-based and routinely combined with group counseling and other psychosocial care. MAT is not a replacement for the group work and the group work is not a replacement for the medication. They do different jobs. If a program tells you to pick one, keep looking.6
Choosing a format that fits your week
Start with the calendar you actually have, not the one you wish you had. If you can name two reliable 90-minute blocks each week—evenings after the kids are down, early mornings before email starts, a recurring lunch hour you can guard—standard outpatient group care under the less-than-9-hours rule is a realistic entry point. If you can name three weekday blocks of three hours each, IOP becomes possible, and the structure tends to hold people who have tried lighter formats and watched them slip.1,2
Then weigh three honest variables:
The first is intensity: how close are you to a recent use, a relapse, or a detox? Closer means more hours, which usually means IOP.
The second is privacy: would walking into a building in your town cost you something professionally? If yes, virtual group care removes that variable entirely while keeping the same regulatory structure.
The third is what else needs attention. Co-occurring depression, anxiety, or a medication question pulls you toward a program that screens, assesses, and coordinates that work alongside the group, rather than treating groups as the whole plan.
A workable first move: pick one format, commit to four weeks, and judge it by whether you are showing up and saying true things—not by whether it feels comfortable. Comfort comes later. If you live in New Hampshire and want virtual group care built around a working schedule, Pathfinder Recovery is one option to consider in that four-state footprint.
Experience Healing With Pathfinder Recovery
If you or a loved one are ready to create a life you love—without having to sacrifice your work, family, and responsibilities—we're here to support you on that journey. Contact us today for personalized care from the comfort of your own home. We will work with your insurance provider so you can focus on what really matters: recovery.
Frequently Asked Questions
What is the difference between outpatient and intensive outpatient (IOP) group therapy in New Hampshire?
The line is set in state rule. Standard outpatient means individual or group counseling totaling less than 9 hours per week. IOP means 9 or more hours per week, plus required screening, treatment planning, individual and group counseling, psychoeducation, and crisis intervention. Outpatient suits stable recovery; IOP fits early recovery or step-down from a higher level of care.1,2
Is group therapy as effective as individual therapy?
For many conditions, yes. A systematic review of group versus individual psychotherapy in adults found that, across multiple mental health diagnoses studied, group and individual therapy did not differ significantly in effectiveness. Group is also the most commonly used format for SUD care in the U.S..9,11
Are virtual group therapy sessions a legitimate option for working professionals in NH?
Yes. New Hampshire's regulatory definitions of outpatient and IOP care apply whether the group meets in a clinic room or on video. A virtual IOP still has to deliver 9 or more weekly hours and the five required clinical services, including group counseling. A virtual standard outpatient group still falls under the less-than-9-hours rule. Licensure and clinical structure do not change.1,2
How is privacy handled in group therapy, especially in a small state like New Hampshire?
Every licensed group operates under confidentiality rules binding the clinician and participants. The facilitator sets ground rules in the first session about what stays in the room, and breaking that agreement is grounds for removal. Virtual groups add control over your physical environment, so colleagues do not see you walk into a clinic. Ask any program directly about camera policy, screen names, and who sees the participant grid.
Where can I access group therapy in New Hampshire if I don't have private insurance?
Start with your regional Community Mental Health Center. New Hampshire's 10 CMHCs cover every county and offer assessment, individual and group therapy, case management, psychiatric services, and 24-hour emergency support, often regardless of insurance status. Hospital behavioral health programs and licensed outpatient providers also accept Medicaid and offer sliding-scale options. Call the CMHC for your county and ask which SUD-focused groups are running this month.4
Can group therapy work alongside medication-assisted treatment (MAT) or care for co-occurring mental health needs?
Yes, and for many people it should. The Surgeon General's review treats MAT and psychosocial care, including group counseling, as complementary parts of evidence-based SUD treatment, not alternatives. NH's IOP rule already requires screening, assessment, and treatment planning that account for co-occurring conditions alongside group work. If a program insists you choose between groups, medication, or mental health care, keep looking.1,6
No items found.
[{"@context":"https://schema.org","@type":"BlogPosting","headline":"Group Therapy in NH: What to Know About Your Options","description":"Explore group therapy options in NH, including program types, confidentiality tips, and how to find care that fits your schedule and treatment needs.","publisher":{"@type":"Organization","name":"Pathfinder Recovery"},"mainEntityOfPage":{"@type":"WebPage","@id":"https://www.pathfinder-recovery.com"}},{"@context":"https://schema.org","@type":"MedicalWebPage","headline":"Group Therapy in NH: What to Know About Your Options","description":"Explore group therapy options in NH, including program types, confidentiality tips, and how to find care that fits your schedule and treatment needs.","mainEntityOfPage":{"@type":"WebPage","@id":"https://www.pathfinder-recovery.com"}},{"@context":"https://schema.org","@type":"FAQPage","mainEntity":[{"@type":"Question","name":"What is the difference between outpatient and intensive outpatient (IOP) group therapy in New Hampshire?","acceptedAnswer":{"@type":"Answer","text":"The line is set in state rule. Standard outpatient means individual or group counseling totaling less than 9 hours per week. IOP means 9 or more hours per week, plus required screening, treatment planning, individual and group counseling, psychoeducation, and crisis intervention. Outpatient suits stable recovery; IOP fits early recovery or step-down from a higher level of care."}},{"@type":"Question","name":"Is group therapy as effective as individual therapy?","acceptedAnswer":{"@type":"Answer","text":"For many conditions, yes. A systematic review of group versus individual psychotherapy in adults found that, across multiple mental health diagnoses studied, group and individual therapy did not differ significantly in effectiveness. Group is also the most commonly used format for SUD care in the U.S.."}},{"@type":"Question","name":"Are virtual group therapy sessions a legitimate option for working professionals in NH?","acceptedAnswer":{"@type":"Answer","text":"Yes. New Hampshire's regulatory definitions of outpatient and IOP care apply whether the group meets in a clinic room or on video. A virtual IOP still has to deliver 9 or more weekly hours and the five required clinical services, including group counseling. A virtual standard outpatient group still falls under the less-than-9-hours rule. Licensure and clinical structure do not change."}},{"@type":"Question","name":"How is privacy handled in group therapy, especially in a small state like New Hampshire?","acceptedAnswer":{"@type":"Answer","text":"Every licensed group operates under confidentiality rules binding the clinician and participants. The facilitator sets ground rules in the first session about what stays in the room, and breaking that agreement is grounds for removal. Virtual groups add control over your physical environment, so colleagues do not see you walk into a clinic. Ask any program directly about camera policy, screen names, and who sees the participant grid."}},{"@type":"Question","name":"Where can I access group therapy in New Hampshire if I don't have private insurance?","acceptedAnswer":{"@type":"Answer","text":"Start with your regional Community Mental Health Center. New Hampshire's 10 CMHCs cover every county and offer assessment, individual and group therapy, case management, psychiatric services, and 24-hour emergency support, often regardless of insurance status. Hospital behavioral health programs and licensed outpatient providers also accept Medicaid and offer sliding-scale options. Call the CMHC for your county and ask which SUD-focused groups are running this month."}},{"@type":"Question","name":"Can group therapy work alongside medication-assisted treatment (MAT) or care for co-occurring mental health needs?","acceptedAnswer":{"@type":"Answer","text":"Yes, and for many people it should. The Surgeon General's review treats MAT and psychosocial care, including group counseling, as complementary parts of evidence-based SUD treatment, not alternatives. NH's IOP rule already requires screening, assessment, and treatment planning that account for co-occurring conditions alongside group work. If a program insists you choose between groups, medication, or mental health care, keep looking."}}]}]
Pathfinder Recovery offers in-home addiction and mental health treatment that fits your life — not the other way around.From at-home detox and MAT to virtual IOP and peer support, our licensed clinicians bring evidence-based care to you through secure telehealth.
The Pathfinder Recovery App and Smart Ring keep your care team connected to your progress between sessions — monitoring sleep, stress, and recovery milestones in real time.It’s proactive, private, and personalized — so support is always within reach.
Virtual Recovery Coaching with Pathfinder Recovery expands access to mental health care online, offering flexible, supportive recovery from anywhere today.
Learn the Buprenorphine Mechanism of Action and how Pathfinder Recovery delivers safe, effective virtual care for opioid treatment and long-term recovery.
Depression In Recovery is supported through Pathfinder Recovery’s virtual care, offering accessible treatment and guidance to strengthen your mental health.