
Navigating Grief and Loss in Recovery
Grief and Loss in Recovery are supported through virtual care at Pathfinder Recovery, offering compassionate guidance that helps individuals heal and rebuild.
November 6, 2025


Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
You already know the basics. You are weighing a decision, not browsing definitions. So here is what matters before you click the intake link.
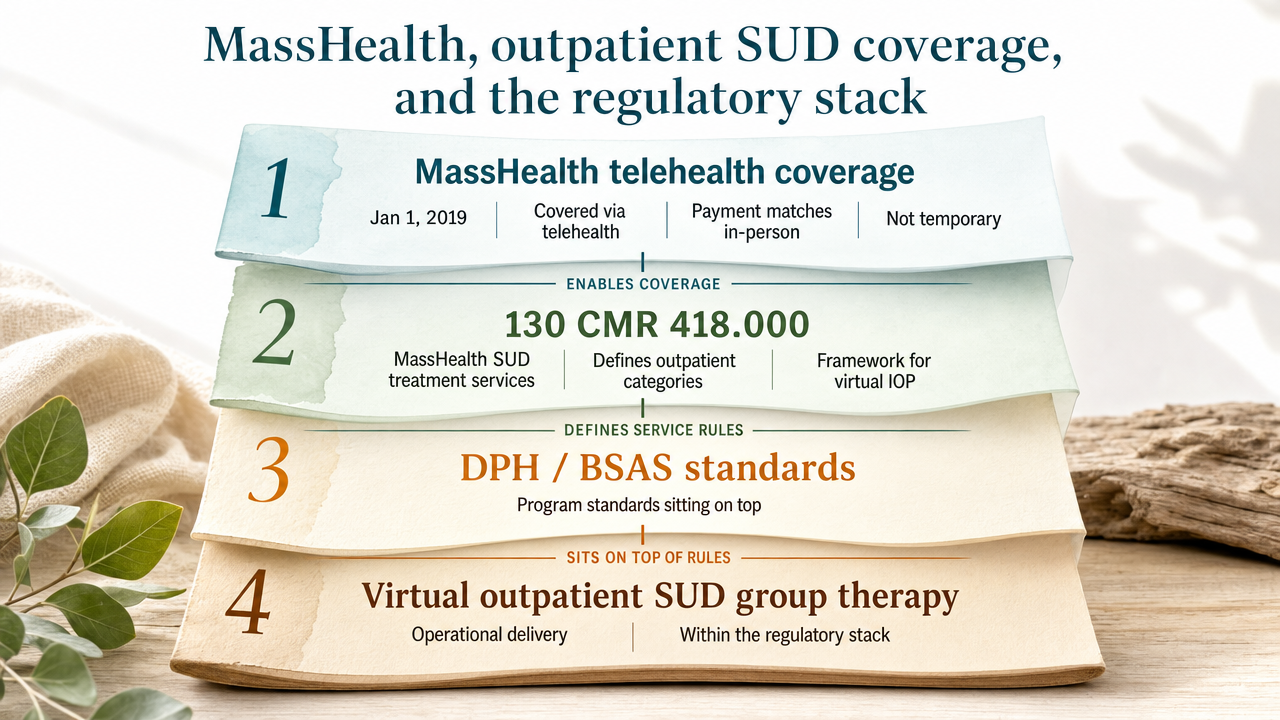
Virtual group therapy in Massachusetts is not a workaround anymore. It is a covered, regulated form of outpatient behavioral health care. State law requires insurers to pay for behavioral health services delivered by interactive audio-video at the same rate as in-person visits 1. MassHealth has allowed outpatient substance use disorder providers to deliver covered services through telehealth since January 1, 2019 2. The service rules sit inside 130 CMR 418.000, and the Department of Public Health publishes Standards of Care that apply whether you are in a room or on a screen 3, 12.
The clinical question is also more settled than it used to be. A 2023 review of telepsychiatry in addiction populations found outcomes similar to in-person care across the studies examined, with the honest caveat that the research base is still smaller than what exists for traditional treatment 7.
That leaves you with the real work: choosing a program that fits a calendar full of meetings, protects your privacy at home and at work, and gives you the structured peer accountability that makes group the most effective recovery modality 8.
The rest of this guide is built around that decision. Coverage. Clinical fit. Calendar fit. Discretion. What separates a good program from a video call with strangers. Showing up to read this far is the work. That counts.
Before 2021, the financial logic of virtual care was murky. A plan might cover a telehealth session at a lower rate, or not at all, or only under emergency rules that could expire. That is no longer how it works in Massachusetts.
Chapter 260 of the Acts of 2020 settled the question. Under state law, behavioral health services delivered by interactive audio-video must be reimbursed at no less than the in-person rate 1. The same parity rule applies to audio-only telephone for behavioral health, which matters on days when your video connection fails or you are taking a session from a quieter spot than your home office.
The statute also defines telehealth broadly. It includes interactive audio-video, remote patient monitoring, audio-only telephone, and online adaptive interviews for mental health and substance use disorder conditions 1. Group therapy delivered over a HIPAA-compliant video platform sits squarely inside that definition.
A few practical consequences flow from this. Your insurer cannot quietly pay your virtual IOP at a discount and pocket the difference. Your copay for a group session should track what you would pay for the same group in a clinic. And the law specifically prevents carriers from using telehealth alone to satisfy network adequacy 1, which means you also retain the right to choose in-person care if you ever want it. The state's later guidance, Bulletin 2021-10, kept that reimbursement framework in place after the early emergency period 11.
So the math is simpler than it used to be. Coverage is the rule, not the exception.
If you have MassHealth, the coverage pathway is even more explicit. As of January 1, 2019, Community Health Centers, Community Mental Health Centers, and outpatient substance use disorder providers may deliver covered services via telehealth, and rates of payment match the in-person rates 2. That predates the pandemic. Virtual outpatient SUD care is not a temporary accommodation in Massachusetts. It is built into the program.
The service rules themselves live in 130 CMR 418.000, the MassHealth regulation governing substance use disorder treatment services 3. That regulation is what defines outpatient SUD service categories, including the structure that a virtual intensive outpatient program follows. Sitting on top of those rules, the Department of Public Health publishes the Bureau of Substance Abuse Services Standards of Care, which sets expectations for treatment quality, clinical documentation, and program operations regardless of whether the service is delivered in person or by screen 12.
Stacked together, the framework looks like this:
You do not need to memorize the citations. You do need to know they exist. When you ask a program about its license, its compliance with state SUD treatment rules, and how it documents your care, you are asking the right questions, and a serious program will answer them without hesitation.
You want a short, honest answer: yes, with caveats worth knowing.
A 2023 review of telepsychiatry in addiction populations looked across the available comparative studies and found outcomes similar to in-person addiction treatment in the studies reviewed 7. That is meaningful. It means the people who showed up for telepsychiatry sessions did roughly as well as the people who showed up in clinic waiting rooms. For a working professional weighing whether a video session is real care, that is the headline.
Here is the caveat the same authors flagged, and it is the one any serious clinician will repeat: the evidence base for tele-addiction care is still smaller than the decades of research behind traditional in-person treatment 7. A 2023 scoping review of telemedicine-delivered SUD treatment reached a similar place. The field is growing fast, feasibility is well documented, and more rigorous comparative trials are still needed to answer the finer questions about which patients do best in which modality 4.
So what does that mean for you on a Tuesday night, debating whether to log in?
It means virtual care is no longer an experimental detour. Federal guidance now describes telebehavioral health as part of an integrated approach to treating substance use disorders, sitting alongside medication management, individual therapy, and peer support rather than substituting for the whole plan 10. It also means the honest unknowns sit at the edges, not the center. Whether a virtual program is right for you depends less on the modality and more on the program's structure, your clinical picture, and whether you actually attend. The research can tell you the door is real. Walking through it is still yours.
There is a quiet assumption that individual sessions are the "real" therapy and group is the warm-up. For substance use disorder care, that has it backwards.
SAMHSA's TIP 41, the federal clinical guidance on group therapy in SUD treatment, treats group as a primary modality. It is where people learn and practice recovery strategies, build interpersonal skills, and strengthen the social support networks that keep recovery going between sessions 8. Individual therapy is valuable. Medication management is often essential. But the mechanism that makes group different, the part you cannot replicate one-on-one, is hearing five or six other adults describe the same Wednesday-night craving you thought was yours alone, then watching them work through it.
That mechanism does not weaken on a screen. The faces are smaller. The accountability is the same. When you say out loud that you are going to skip the work happy hour on Thursday and three people ask you on Monday how it went, the structure is doing what it is designed to do.
Group is also where skills get rehearsed in close to real time. Refusal language. Boundary scripts with a partner or a boss. The two-sentence answer you will give the colleague who asks why you are not drinking. Those are not insights you generate alone at midnight. They are lines you try out in front of other people who will be honest about whether they land.
If you are choosing between a program that centers group and one that treats it as a bolt-on, the research points you toward the first.
The expansion of virtual care here was not a marketing trend. It was a response to two pressures that landed on the state at the same time.
The first was demand. Massachusetts grew from 7,066,568 residents on July 1, 2023 to 7,136,171 on July 1, 2024, a gain of 69,603 people in a single year 13. That kind of growth sits on top of a behavioral health system that was already running tight. Waitlists for outpatient SUD care in some parts of the state have been measured in weeks, not days. For a working professional, a four-week wait usually means the moment passes and you do not start.
The second pressure was structural. Once it was clear that interactive audio-video could carry a real clinical session, facilities moved fast. Telehealth availability at substance use disorder treatment facilities increased by 143% from 2020 to 2021 5. Worth being precise about what that number is and is not: it measures facility-level adoption of the service modality, not how many patients used it or how well they did. It tells you the shelves got stocked, not how many people bought what was on them.
For you, the practical effect is straightforward. The supply of virtual outpatient SUD care in Massachusetts is wider than it was five years ago, and the calendar barriers that used to be the dealbreaker have eased. A 7 pm group exists somewhere on a Tuesday. So does a noon one. The question is which program is built well enough to be worth your evening.
The calendar is usually what kills treatment for working professionals. A 2 pm group on a Wednesday is not a real option when you have a standing client call and a manager who notices empty chairs. Virtual programs solved that problem in a specific way: they built cohorts around the hours when your work day is not watching.
A typical virtual intensive outpatient program runs about nine to twelve clinical hours a week, spread across the week instead of stacked into a clinic day. The structure most often looks like three group sessions of roughly 90 minutes each, one individual therapy session, and a peer coaching touchpoint. Group is the spine because group is where the work happens: SAMHSA's clinical guidance on group therapy frames it as the modality where people learn and practice recovery strategies, build interpersonal skills, and strengthen the social support networks that hold recovery together between sessions 8.
The hours are where the design gets useful. Lunch-hour cohorts run 12:00 to 1:30 on Mondays, Wednesdays, and Fridays. Evening cohorts run 6:00 or 7:00 to 8:30. Some programs offer early-morning groups before the inbox opens. The point is not novelty. The point is that the three or four hours of group you need each week can sit inside the hours when your calendar is already yours.
A sample week might look like this: Monday 7:00 pm group, Wednesday 12:00 pm group, Thursday 5:30 pm individual session, Friday 7:00 pm group, Sunday 11:00 am peer coaching. Five touchpoints. Zero conflicts with the 9-to-6. The structure works because it was built for people who cannot move their workday.
Yes, signing into a group of strangers from your kitchen feels strange the first time. The discretion questions are real, and they are answerable.
Start with the room. A door that closes is the single most useful piece of equipment you own. If you do not have one, a parked car with the engine off works. Headphones with a microphone keep the other voices private; built-in laptop speakers do not. Position the camera so what is behind you is a wall, a curtain, or a bookshelf, not a hallway where someone might walk through.
The screen during group is usually less exposing than people expect. Most platforms show a grid of small video tiles with first names or initials. You can typically rename yourself, blur or replace your background, and use the chat for things you do not want to say out loud yet. Massachusetts requires providers to use HIPAA-compliant technology and to handle consent and documentation the same way they would for an in-person visit 2, so the platform itself is not a leak point a serious program would tolerate.
Insurance is the question people forget to ask until the envelope arrives. Explanations of benefits go to the policyholder's address. If you are on a spouse's plan or a parent's plan, ask the program's billing team how the service is coded and what shows up on an EOB. You can usually request electronic-only statements or update the mailing preference with your carrier.
Privacy is a setup, not a hope.
A Zoom link is not a program. The difference between real care and a video call with strangers shows up in details you can ask about before you ever log in.
Start with the clinical structure. A serious virtual program in Massachusetts operates inside 130 CMR 418.000 and the DPH Bureau of Substance Abuse Services Standards of Care, which set expectations for assessment, treatment planning, documentation, and continuity 3, 12. That means an intake that takes more than fifteen minutes. A written treatment plan you can see. Licensed clinicians, not just facilitators. Ask who runs your group and what credential they hold. If the answer is vague, the program is too.
Look at how group is built. SAMHSA's clinical guidance treats group as the modality where people learn skills, practice them, and reinforce social support 8. That requires a stable cohort, not a rotating drop-in. Closed or semi-closed groups of six to ten members, the same faces most weeks, are doing different work than an open room of twenty.
Ask about the integration. Federal guidance frames telebehavioral health as part of a coordinated SUD plan, not a standalone product 10. A quality program connects your group work to individual therapy, peer coaching, and medication management when it is indicated, with one record and one team that talks to each other. If group sits in a silo, you are getting a piece, not a plan.
The platform should be HIPAA-compliant and named, with consent and documentation handled the way an in-person clinic would 2. And the program should be honest about who it serves well and who it does not. Quality sounds like specificity. Sales sounds like everything.
Honesty about the limits is part of how you choose well. A few lines worth drawing clearly.
Virtual group therapy is not primary mental health care. If your main clinical need is treatment for a standalone psychiatric condition without a substance use component, this is not the right door. Where it fits is alongside SUD treatment, with co-occurring anxiety, depression, or trauma supported as part of an integrated plan 10.
And it is not equally accessible to everyone. A 2024 review of telehealth and behavioral health equity found persistent gaps in access tied to broadband, devices, language, and private space at home 6. If you do not have a quiet room or a reliable connection, the modality itself becomes a barrier. That is worth naming out loud, not engineering around with optimism.
Knowing what virtual group will not do for you is how you protect what it can.
The first two weeks decide more than people expect. Not because the work gets easier, but because the habit of showing up either takes hold or it doesn't. A few specific moves help.
Before the first session:
During the first two weeks:
Showing up to session one is the work. Showing up to session six is recovery starting to hold. Both count. If you live in Massachusetts and want a program built around a working schedule, Pathfinder Recovery is one place to start that conversation.
Yes. Under Chapter 260 of the Acts of 2020, behavioral health services delivered by interactive audio-video must be reimbursed at no less than the in-person rate 1. MassHealth has paid outpatient SUD providers for telehealth-delivered covered services at in-person rates since January 1, 2019 2. Your copay should track what you would pay in clinic.
Not from the program itself. Massachusetts requires HIPAA-compliant technology and the same consent and documentation standards as in-person care 2. The exposure points are practical: where the EOB envelope arrives, what shows up on a shared family plan, and whether your home setup is private. Ask the billing team about coding and request electronic statements from your carrier.
For addiction populations, a 2023 telepsychiatry review found outcomes similar to in-person care across the studies examined, with the caveat that the evidence base remains smaller than for traditional treatment 7. A 2023 scoping review of telemedicine SUD care reached similar conclusions on feasibility while flagging the need for more comparative trials 4. What matters most is program structure and whether you attend.
Most programs build cohorts around lunch hours and evenings. A typical week runs about nine to twelve clinical hours, usually three 90-minute groups plus one individual session and a peer coaching touchpoint, grounded in SAMHSA's framing of group as the modality for skills practice and peer support 8. Lunch cohorts run 12:00 to 1:30. Evening cohorts run 6:00 or 7:00 to 8:30.
Three groups. People whose primary need is standalone psychiatric care without a substance use component belong in a different setting; virtual SUD programs treat co-occurring mental health alongside addiction, not as primary care 10. People with active alcohol or benzodiazepine dependence need medically supervised detox first. And people without reliable broadband, a private room, or a working device face real access barriers documented in the equity research 6.
Ask four things. Does the program operate inside 130 CMR 418.000 and the DPH Standards of Care, with licensed clinicians running group 3, 12? Is group built as the spine of treatment, with stable cohorts of six to ten members 8? Is it integrated with individual therapy, peer coaching, and medication management when it is indicated 10? And is the platform HIPAA-compliant and named 2?
November 6, 2025

November 7, 2025

May 26, 2026