
Virtual Recovery Support in MA for Professionals
Learn how Massachusetts professionals can access flexible, confidential recovery support virtual MA services with telehealth parity and remote care options.
May 26, 2026


Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
If you're reading this between meetings, you already know the hard part isn't believing recovery is possible — it's protecting the time and privacy to keep doing the work after primary treatment ends. The good news: what's available in Massachusetts right now is genuinely different than it was even eighteen months ago. A December 2024 state law expanded insurance coverage for recovery coach services and made opioid reversal medication available without cost-sharing or prior authorization. MassHealth continues to support behavioral health telehealth, including for substance use disorder care. And the Bureau of Substance Addiction Services oversees a statewide network of peer-led, free drop-in centers that exist outside the clinical system entirely.2,4,7,8
What that means for you: ongoing support is no longer a single thing you sign up for. It's a stack you assemble. This guide maps the formats, what the evidence actually says about each, and how to fit them around a calendar that doesn't bend easily. No 101 on what addiction is. You're past that.
Two changes from the December 2024 law are worth knowing before you plan anything else. First, all health plans in Massachusetts now have to cover opioid reversal drugs without cost-sharing or prior authorization. That means naloxone in your bag, your partner's bag, your office drawer — without a copay conversation, without faxed paperwork, without a pharmacist call to your insurer. If you've been quietly paying cash to avoid a claim trail, that calculation has shifted.2
Second, and this is the bigger structural change: health plans must now cover recovery coach services at no less than MassHealth rates. Recovery coaching used to live in a strange place — sometimes free through a community program, sometimes out-of-pocket at rates that made it feel like a luxury. Now it's a covered benefit on the same footing as other behavioral health services. The law also formalizes recovery coach licensure, which matters because it gives plans and employers a credentialed category to reimburse against.2
For you, the practical effect is that a weekly check-in with a trained coach — someone who isn't your therapist, isn't a doctor, and has lived experience with recovery — is now a benefit you've likely been paying premiums for without using. If you're finishing IOP or stepping down from residential care, this is the piece of the stack that got dramatically cheaper this year.
Here's something the headlines undersell: Massachusetts opioid-related overdose deaths fell about 10% in 2023 compared with 2022, and provisional data showed a continued decline of roughly 9% in early 2024. Two consecutive years of measurable improvement, after a decade of mostly the opposite direction.6
That isn't a victory lap. People are still dying, and the people closest to this work will tell you so. But if you've been carrying the quiet weight of "recovery doesn't really work at the population level," the data is starting to push back on that. Better access to medication for opioid use disorder, wider naloxone distribution, and a steadier recovery support infrastructure all show up in numbers like these — even if no single intervention gets the full credit.6
Why this matters for how you plan your own stack: the state didn't expand recovery coach coverage and telehealth flexibilities in a vacuum. Those policy choices sit on top of a system that is, by its own surveillance data, starting to bend. You're not signing up for a hopeful experiment. You're plugging into a network that's been quietly producing better outcomes for two years running.

The other side of that improving trend: in 2024, Massachusetts recorded 1,646 unintentional and undetermined intent drug overdose deaths, a rate of 22.8 per 100,000 residents. That figure is why the recovery support menu exists at the scale it does — peer centers in most regions of the state, telehealth coverage written into MassHealth bulletins, a December 2024 law with bipartisan momentum behind it.5
It also tells you something quieter. If you're a working professional in recovery, you are not a rare case the system is figuring out how to serve. You're part of a population large enough that the state has invested in formal infrastructure — licensing, reimbursement rules, drop-in centers, virtual modalities — to support continued recovery after primary treatment ends. The privacy concerns you have are not unusual. The schedule constraints you have are not unusual. The need for ongoing, lower-intensity support is the baseline, not the exception.4,5
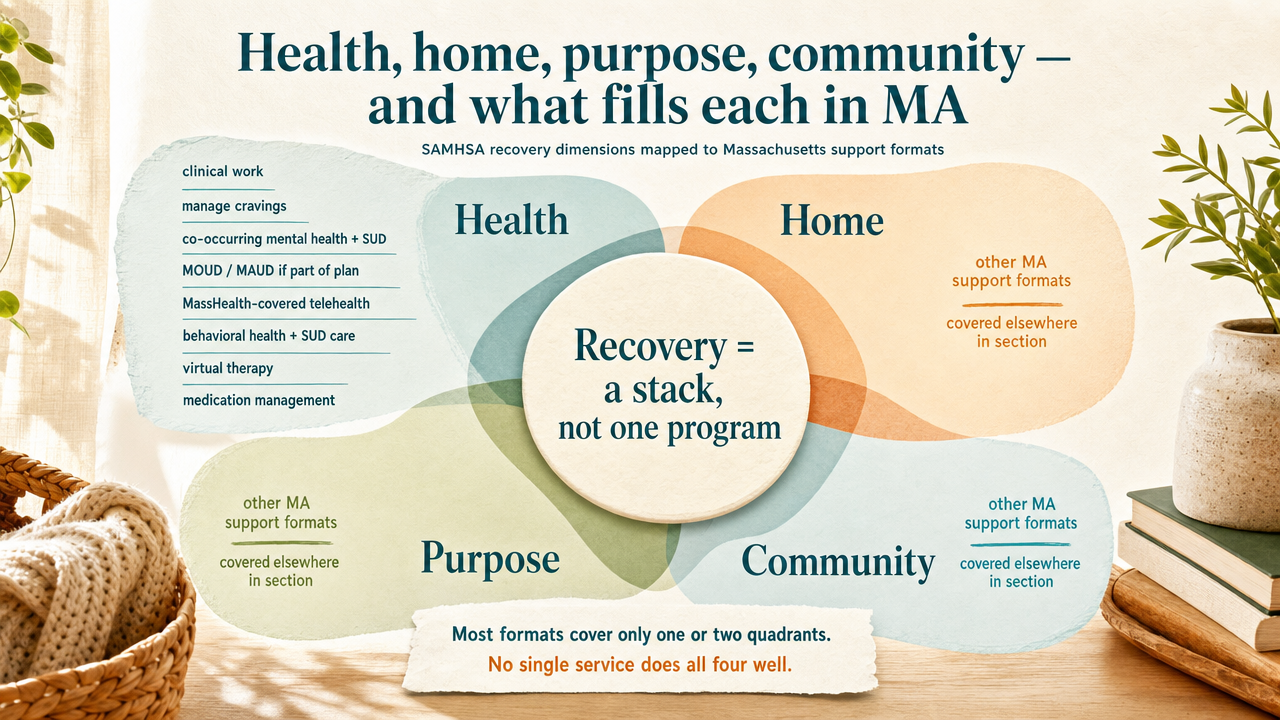
SAMHSA defines recovery as a process of change across four dimensions: health, home, purpose, and community. It sounds abstract until you try to assemble your own support and realize most of the formats on offer only cover one or two of those quadrants. That's why people in long-term recovery talk about a stack instead of a program — no single service does all four well.14
Here's how the Massachusetts menu maps onto each dimension:
Look at your current week. Which quadrants are covered, which are thin, which are empty? That's your planning question. The sections ahead match specific formats to the gaps.
Peer Recovery Support Centers (PRSCs) are the part of the Massachusetts menu that most working professionals overlook, usually because the format doesn't look like a service in the traditional sense. There's no intake, no co-pay, no clinical record. They're free, peer-led community spaces where people in or seeking recovery — and their families — can drop in for support groups, social activities, recovery coaching, and linkage to other services. BSAS funds and supports them as part of the statewide recovery system.4,8
What you actually get when you walk in: a quiet room with coffee, a posted schedule of peer support meetings, people who have been where you are and don't need it explained. Some centers run evening and weekend hours specifically because people work during the day. Nothing you say there becomes part of a medical chart, because there is no chart.8
The honest limitation: a PRSC is not clinical care. It doesn't replace therapy, medication management, or a structured aftercare program. Think of it as the community quadrant — a place to belong that exists outside both the treatment system and your professional life.
A recovery coach is not your therapist and not your sponsor. They're a trained, increasingly credentialed peer who works with you on the practical mechanics of staying in recovery — values, goals, routines, the awkward conversations you've been putting off, the relapse warning signs you've stopped noticing. The 2021 review of recovery support services found that peer coaching is associated with better engagement and lower relapse risk, while also noting the evidence base is still maturing.13
The reason this format moved up most professionals' shortlist in 2025: the December 2024 Massachusetts law requires health plans to cover recovery coach services at no less than MassHealth rates, and it formalizes coach licensure. A weekly thirty-minute call that used to be an out-of-pocket line item is now a covered behavioral health benefit, with a credentialed provider category behind it.2
What coaching does well: continuity between clinical appointments, accountability that doesn't feel like surveillance, and a person who can take a Tuesday-night call when something at work has knocked you sideways. What it does not do: diagnose, prescribe, or treat co-occurring mental health conditions. Those still sit with a clinician.
Virtual continuing care is where the clinical pieces of your stack live after primary treatment ends — individual therapy, group therapy, medication management for opioid or alcohol use disorder, integrated support for co-occurring mental health conditions — delivered through video or phone instead of an office visit. MassHealth's behavioral health telehealth bulletin covers SUD treatment across audio and audiovisual modalities, which is what allows facilities to bill for the visit you take from your home office. Research on state telehealth policy environments found that this kind of permissive posture meaningfully increases the likelihood that SUD facilities actually offer telehealth in the first place.7,11
For a professional calendar, the scheduling math is the headline. A virtual IOP step-down group at 7 p.m., a thirty-minute therapy session in the gap between two meetings, a psychiatrist appointment that doesn't require a half-day off — all of it from a closed door. The CDC's review of pandemic-era telehealth expansion documented that virtual delivery improved access to medications for opioid use disorder and counseling, particularly for people who had previously faced commute, time, or geographic barriers.12
Where it has limits: the evidence on digital recovery support is promising but still developing, and not every clinical encounter belongs on video. The first months of detox stabilization, certain crisis situations, and some psychiatric assessments still call for higher-intensity in-person care.10
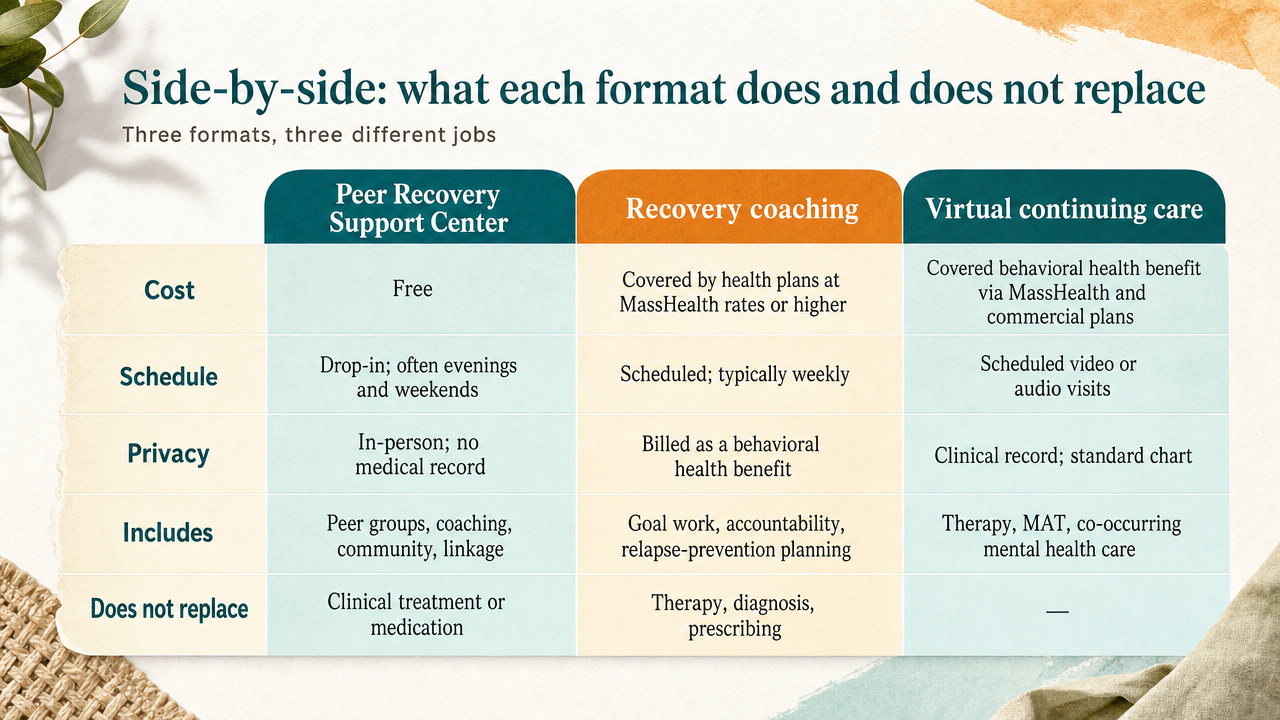
Three formats, three different jobs. Holding them next to each other makes the assembly question easier:
Most working professionals end up using two or three of these, not one. The coaching call protects the week. The virtual clinical visits handle the medical pieces. The PRSC drop-in, when you can make it, gives you a community that isn't tied to a billing code.
The privacy question isn't paranoid — it's a planning input. Different formats leave different trails, and knowing which is which lets you stop guessing.
Clinical care, whether in person or virtual, generates a medical record. Your therapy session, your medication management visit, your virtual IOP group — all of those produce chart notes, diagnosis codes, and claims that move through your insurance. That's true regardless of whether you turn your camera on. The MassHealth behavioral health telehealth bulletin permits both audio-only and audiovisual modalities for SUD treatment, which means if you're in a shared workspace or a parked car between appointments, audio-only is a real option without compromising the visit's billable status.7
Recovery coaching is now a covered behavioral health benefit under the December 2024 law, so if you're using insurance to pay for it, expect the same chart-and-claims trail as therapy. If you'd rather keep coaching outside your insurance entirely, that's still a choice — some people pay cash specifically to keep it off the record.2
Peer Recovery Support Centers sit on the other end. They're free, peer-led, and nonclinical, with no medical record produced from your participation. Nothing you say at a drop-in group becomes a chart note. For some readers, that's the whole appeal.8
Here's what a layered week can actually look like for someone with a full calendar. Not a prescription — a sketch.7,8
That's four touchpoints, roughly three hours total, two of them at home, one during the workday, one on the weekend. No commute except the Saturday drop-in. Nothing visible to your employer. Three of the four are covered benefits; the fourth is free. Adjust the mix to your own life — the point isn't this exact schedule, it's that the formats now exist to build one.
Here's the honest version, because you'd spot a sales pitch from a mile off. The peer-reviewed review of online digital recovery support services concludes that these tools are promising and increasingly available, but the evidence base on comparative effectiveness, engagement patterns, and optimal service design is still developing. That's not a reason to skip virtual aftercare. It's a reason to use it with your eyes open.10
What's better established: the broader category of recovery support services — peer coaching, recovery community centers, mutual help, recovery housing — is associated with improved substance use outcomes, better engagement, and lower relapse risk in the 2021 review of the field, with the same caveat that methodological gaps remain. And the CDC's analysis of pandemic-era telehealth expansion documented real access gains for medications for opioid use disorder and counseling, particularly for people who previously hit commute, time, or geographic walls.12,13
The practical read: virtual aftercare is not a downgrade from in-person care for most of what you'll need after primary treatment. It's a format change with a maturing evidence base. Use it where the format helps — therapy, coaching, groups, medication management — and don't expect it to do the things video isn't built for.
Here's what the money actually looks like for each piece of the stack in Massachusetts right now, using only what's written into law and policy.
Start with the quadrant that's thinnest right now, not the format that sounds most familiar. If your clinical care is solid but you're isolated, the gap is community — a Peer Recovery Support Center drop-in or an online mutual-help meeting belongs on your calendar this week. If you're connected but drifting on goals and warning signs, recovery coaching is the piece that just became a covered behavioral health benefit and is built exactly for that work. If therapy and medication management feel scattered, virtual continuing care consolidates them into something that fits between meetings.2,7,8
Pick one addition. Schedule it. The stack gets built one slot at a time, and the formats are finally there to support a calendar like yours.
For questions and support on your recovery journey—with real world support that doesn't require you to leave your home—call Pathfinder Recovery today.
Yes. The December 2024 state law requires health plans in Massachusetts to cover recovery coach services at no less than MassHealth rates, and it formalizes recovery coach licensure so plans have a credentialed provider category to reimburse. If you have insurance here, recovery coaching is now a covered behavioral health benefit you've been funding through premiums.2
A Peer Recovery Support Center (PRSC) is a free, peer-led community space where people in or seeking recovery, along with their families, can drop in for support groups, social activities, recovery coaching, and linkage to other services. There's no intake, no fee, no medical record. BSAS supports a statewide network of these centers, and many run evening and weekend hours.4,8
Yes. MassHealth's behavioral health telehealth bulletin covers SUD treatment across both audio-only and audiovisual modalities, which is what allows providers to deliver therapy, group work, and medication management visits to your home. Commercial plans largely follow the same posture. Research on state telehealth policy environments confirms this kind of permissive approach measurably increases the share of SUD facilities offering virtual care.7,11
A recovery coach is a trained, credentialed peer who works with you on goals, routines, accountability, and relapse warning signs — not diagnosis or prescribing. Therapy and medication management remain with licensed clinicians and address mental health conditions, trauma, and pharmacotherapy. Coaching fills the space between clinical appointments. Most working professionals end up using both, because they do genuinely different jobs.2,13
The honest answer: the evidence is promising but still developing. A peer-reviewed review of digital recovery support services found these tools are increasingly available and useful, while noting comparative effectiveness research is still maturing. The CDC's analysis of pandemic-era telehealth expansion documented real access gains for medications for opioid use disorder and counseling. Virtual works well for most aftercare, not crisis stabilization.10,12
Different formats leave different trails. Clinical visits — therapy, medication management, virtual continuing care — produce chart notes and insurance claims, though MassHealth permits audio-only modalities so you don't need video from a shared space. Recovery coaching billed through insurance follows the same pattern; cash-pay coaching does not. PRSC drop-ins are nonclinical and produce no medical record at all.7,8
May 26, 2026

November 6, 2025

November 7, 2025