Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
Key Takeaways
Massachusetts built a dedicated peer recovery layer for months two through nine, with CARC credentialing and a MassHealth benefit covering coaches who have at least two years of their own recovery 1, 2.
CARC certification requires 500 supervised work hours, 60 education hours, and 35 supervision hours, with 30 continuing education hours every two years — verify renewal status when vetting a coach 2.
Stack a coach with a Peer Recovery Support Center or Recovery Learning Community based on geography and co-occurring needs; virtual coaching works well for Western and Central MA schedules 5, 6.
Call your MassHealth MCO or Behavioral Health vendor to ask which contracted providers offer Recovery Coach Services under H2016-HM, then interview one or two coaches using a fit-focused checklist 1.
The Aftercare Gap Most People Hit in Months 2–9
You finished the structured part. Detox, inpatient, IOP, residential — whatever combination you stacked, the part with a daily schedule and people checking on you is behind you. The first few weeks home felt different. Sharper. You were paying attention. Then somewhere around week six or eight, something quieter set in.
This is the window most treatment veterans in Massachusetts describe the same way: months two through nine, when the scaffolding is gone but the brain is still rewiring. Your therapist may be down to every other week. The group chat from rehab has gone quiet. Work has expectations again. And the cravings, when they come, do not announce themselves on a Tuesday at 10 a.m. when your clinician is available.
This is the gap. It is not a personal failure. It is a design problem in how care gets handed off. Massachusetts has spent the last several years building a layer specifically for this stretch — credentialed peer recovery coaches, peer-led support centers, and a MassHealth benefit that pays for the work 1, 5. SAMHSA describes peer coaching as non-clinical support for long-term recovery, which is the exact part of the arc that clinical aftercare alone tends to under-cover 10.
The rest of this guide maps what is actually available to you in Massachusetts, how to vet it, and how to stack it with the clinical care you already have. No fear hooks. No selling you on something you do not need.
What a Peer Recovery Coach Actually Does in Massachusetts
The Non-Clinical Scope, Defined
A peer recovery coach is not your therapist. Not your sponsor. Not a case manager with a clipboard checking boxes. The federal definition, the one Massachusetts builds its benefit on, is specific: peer recovery coaches provide non-clinical assistance to support long-term recovery from substance use disorders 10. That word — non-clinical — is doing a lot of work.
What it means in practice: a coach walks alongside you. They have at least two years of their own sustained recovery, which MassHealth requires before anyone can bill for the service 1. They have lived the months you are living now. They use that experience to help you set recovery goals you actually care about, connect you to community spaces, troubleshoot the logistics that keep tripping you up — a ride to a meeting, a conversation with HR, a plan for the family wedding in August.
What it does not mean: a coach will not diagnose you, prescribe anything, deliver psychotherapy, or manage a crisis on their own. If you are in acute danger, they help you get to the people who handle that. If you need medication adjustments, they help you get to your prescriber. The boundary is the point. The coach holds the long arc of recovery while clinicians handle the clinical work.
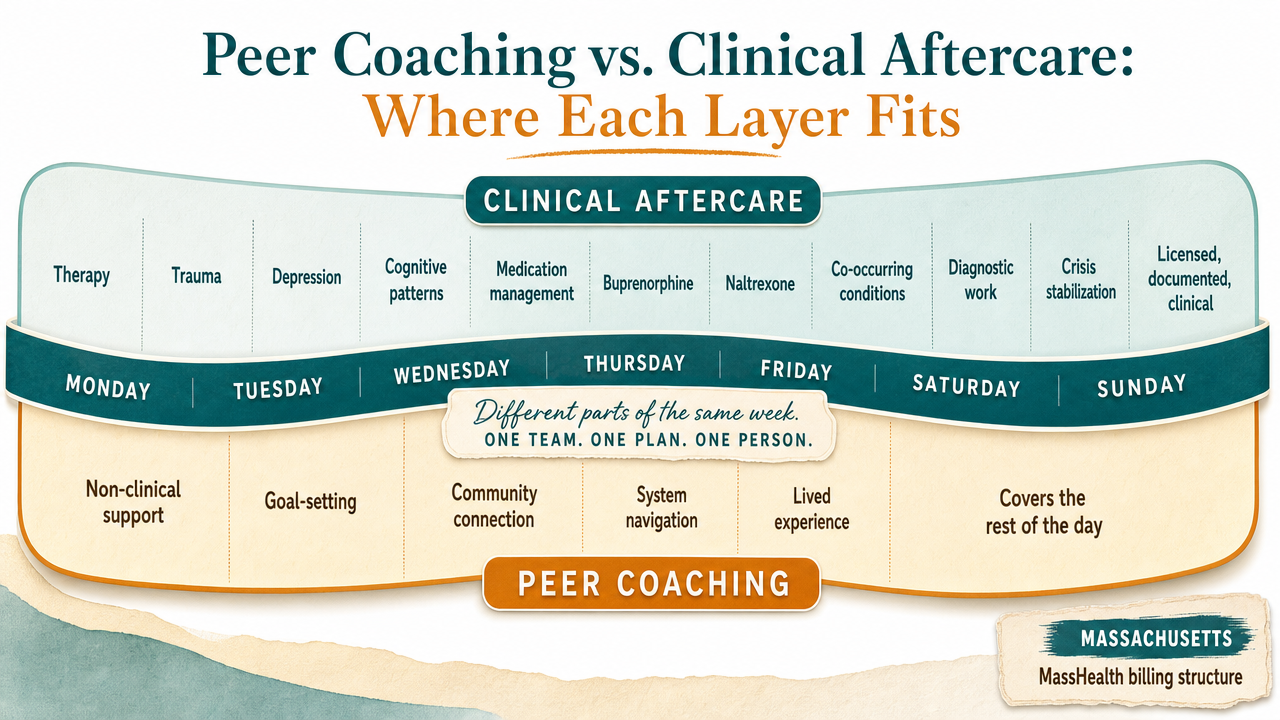
Peer Coaching vs. Clinical Aftercare: Where Each Layer Fits
Most treatment veterans already know this intuitively, but it helps to see it laid out. Peer coaching and clinical aftercare are not competing options. They cover different parts of the same week.
Clinical aftercare is what your therapist, prescriber, and psychiatrist provide. Therapy sessions for trauma, depression, and the cognitive patterns underneath your use. Medication management for buprenorphine, naltrexone, or co-occurring conditions. Diagnostic work. Crisis stabilization when something goes sideways. That work is licensed, documented, and clinical in scope.
Peer coaching covers the rest of the day. SAMHSA frames the peer role as non-clinical support across four practical functions: goal-setting, community connection, system navigation, and modeling recovery through lived experience 10. In Massachusetts, MassHealth pays for this work under procedure code H2016-HM on a daily case rate structure, which means the coach gets reimbursed for the day's contact rather than billing every fifteen minutes like a therapist would 1. That billing design tells you something about how the role is meant to function — flexible, responsive, woven into the texture of your week rather than slotted into a 50-minute hour.
Here is the way to hold it in your head. If something is happening inside your nervous system — a panic attack, a depressive episode, a craving so loud it feels like its own voice — the clinical layer is built for that. If something is happening in your week — a job interview Tuesday, a family member who keeps texting, a Saturday with no plans — the peer layer is built for that. You need both. Most people leaving structured care have the clinical layer set up and the peer layer missing, which is exactly why months two through nine feel so exposed.
How Massachusetts Credentials Recovery Coaches (CARC)
The Hours Behind the Credential
When you are vetting a coach, the credential to ask about is CARC — Certified Addiction Recovery Coach. Massachusetts built it so the title means something concrete instead of whatever a website wants it to mean.
The state requires three things before someone can hold the credential, and the numbers are worth knowing because they tell you what kind of preparation sits behind the person on the other side of your video call. An applicant needs 500 hours of supervised work experience, 60 hours of education, and 35 hours of direct supervision before they can sit for initial certification 2. That is not a weekend workshop. It is closer to a full academic year of structured work, with someone watching, teaching, and signing off.
The certification is good for two years. To recertify, a coach has to complete 30 contact hours of approved continuing education, which keeps them current on practice standards, ethics, and the boundaries of the role 2. If a coach you are talking to cannot tell you when their CARC was last renewed, that is information.
The reason this matters for you: peer coaching is built on lived experience, but lived experience alone does not teach someone how to hold space without projecting their own story onto yours, how to refer out when something clinical is happening, or how to document a session in a way that protects your confidentiality. The hours behind the credential are how the state translates lived experience into a professional discipline. When you ask a coach about their CARC, you are not being skeptical. You are doing the same due diligence you would do with any other person you let into a hard part of your life.
Breakdown of the hours required for initial CARC certification in Massachusetts, covering supervised work experience, education, and direct supervision.
The 2024 Licensure Shift and What It Doesn't Yet Mean
Massachusetts is in the middle of moving recovery coaching from certification toward formal licensure. The Recovery Coach Commission — the state body charged with reviewing training and recommending standards — has been the engine behind this shift, building on the same policy track that produced the MassHealth benefit 3. MassHealth has also held listening sessions and invited written stakeholder feedback to shape how the program evolves 4.
Here is what that means for you right now: not as much as the headlines suggest. Licensure changes the regulatory floor a coach has to stand on, and over time it will probably tighten scope-of-practice boundaries, complaint processes, and insurance coverage beyond MassHealth. It does not change the day-to-day work of coaching, and it does not invalidate the CARC credentials already in the field. The coach you find this month is still working under the same standards they worked under last month.
If you want to track the shift, the Recovery Coach Commission page and MassHealth's stakeholder updates are the two places where real changes will surface first 3, 4. Anything else you read about the law is interpretation. For your aftercare plan, the practical move is the same one you would have made before the law passed: find a CARC-certified coach, ask about their supervision, and trust the credential the state is actually issuing today.
How MassHealth Pays for Peer Coaching
Eligibility, the Two-Year Recovery Standard, and Billing Mechanics
If you are enrolled in MassHealth, peer recovery coaching is a covered benefit. That sentence does a lot of practical work, so it is worth slowing down on what it actually means.
Eligibility on your side is straightforward. MassHealth covers Recovery Coach Services for members seeking to achieve or maintain recovery from a substance use disorder 1. You do not need to be at a specific point in the arc — newly discharged, six months in, two years in, returning after a setback. The benefit is built for the long stretch, not just the first ninety days.
Eligibility on the coach's side is where the standards tighten. To be a qualified coach billing under MassHealth, a person must have at least two years of their own sustained recovery1. That requirement is not arbitrary. It is the state saying lived experience has a floor, and the floor is two years. If someone is offering coaching with less than that, they may be doing good work, but they cannot bill the benefit for it.
The billing mechanics shape the experience more than most people realize. MCOs, ACPPs, and the Behavioral Health vendor pay for coaching using procedure code H2016-HM on a daily case rate structure1. A daily case rate means the coach is reimbursed for the day's contact, not in fifteen-minute increments. For you, that often translates to a coach who can pick up the phone when you actually need them — a Sunday afternoon, a stretch between sessions, the hour before a hard family dinner — without watching a clock.
Why the Benefit Is Structured Through Medicaid
The reason peer coaching sits inside MassHealth rather than as a standalone state grant is partly historical and partly strategic. Medicaid programs across the country cover recovery support services — peer support, supportive housing, supported employment, skills training — because these supports keep people connected to treatment and reduce the cost of preventable crises 12. Massachusetts followed that pattern, then went further with a defined benefit, a coverage policy, and a credentialing standard tied to it.
Routing coaching through MassHealth does two things for you. It makes the service free at the point of contact if you are a member, no separate bill and no sliding scale to negotiate. And it forces the work into a documented, contracted system, which means the coach you connect with is part of a network with supervision and standards behind it, rather than a freelance arrangement with nothing holding the quality line. The MACPAC framing of recovery supports as a Medicaid-covered category is the policy logic behind that design 12.
Recovery, Made Possible — From Home
Pathfinder Recovery offers in-home addiction and mental health treatment that fits your life — not the other way around. From at-home detox and MAT to virtual IOP and peer support, our licensed clinicians bring evidence-based care to you through secure telehealth.
The Massachusetts Peer Ecosystem Beyond One-on-One Coaching
Peer Recovery Support Centers and Recovery Learning Communities
A coach is one layer. The state has built a few more around it, and the people who do well in months two through nine usually have at least two of them stacked together.
Peer Recovery Support Centers are the most concrete piece. They are free, peer-led physical spaces scattered across Massachusetts where people in recovery from substance use can drop in, attend meetings, take a coffee, use a computer, or sit with someone who gets it 5. No appointment, no intake form for most activities, no insurance card. You walk in. That low threshold matters when your Saturday feels long and your apartment feels small. The centers run mutual-aid groups, social events, wellness activities, and warm hand-offs to other services when you need them.
Recovery Learning Communities operate on a related but distinct track. RLCs are peer-run networks built around self-help, information and referral, advocacy, and training — historically rooted more in the mental health peer-support tradition, with substance use overlap 6. If you have a co-occurring condition, RLCs often have programming and trained peers who understand that intersection in ways a substance-use-only space might not. Several RLCs in Massachusetts also offer virtual peer support, which is useful if you are in a region without a brick-and-mortar center nearby.
The way these pieces fit together is the part to hold onto. A CARC-certified coach gives you a one-on-one relationship. MassHealth pays for that work through the H2016-HM benefit if you are a member 1. The peer recovery support center gives you a community space and ambient connection 5. The Recovery Learning Community gives you advocacy, training, and peer support that often crosses over into mental health 6. None of them replace clinical care. Together they form the layer that holds the week when the clinical hour ends. You do not need all four lit up at once. Most people start with a coach plus one community space and add the rest as the year goes.
Specialized Tracks: Older Adults and Other Workforce Niches
The peer workforce in Massachusetts is not one uniform role. The state has started building specialized tracks for populations whose recovery looks different from a 30-year-old leaving IOP.
The Certified Older Adult Peer Specialist training is one example worth knowing about. It prepares Certified Peer Specialists and Recovery Coaches age 50+ to work with older adults in recovery — a population whose substance use patterns, medication interactions, grief load, and social isolation pressures do not map neatly onto a general coaching curriculum 13. If you are over 50, or you are helping a parent who is, asking whether a coach has this specialization is a fair and useful question.
The broader point is that you can ask about fit, not just credentials. Coaches bring different lived experience — opioid use disorder versus alcohol, parenting in recovery, military background, LGBTQ+ identity, return after a long stretch out. A good matching conversation surfaces that early so the coaching relationship can carry weight when you actually need it.
Virtual Peer Coaching for Real Massachusetts Schedules
If you live in Western or Central Massachusetts, or you are juggling a job that does not respect a 3 p.m. appointment, the geography of in-person coaching can quietly become the reason you stop showing up. A coach in Boston is not useful when you are in Pittsfield on a Wednesday. A 4 p.m. session in Worcester is not useful when your shift ends at 5:30.
Virtual peer coaching solves a logistics problem, not a clinical one. The work itself — goal-setting, lived-experience modeling, helping you think through the Saturday that scares you — translates well over a video call or a phone, because the substance of the relationship is the conversation 10. The MassHealth benefit was designed with this in mind. Because reimbursement runs on the H2016-HM daily case rate rather than a per-minute clock, a virtual coach can pick up when something is actually moving in your week — a text on a lunch break, a call the night before a court date, a longer Sunday session when you have the time 1.
A few things to keep in mind when you set this up. Ask whether the coach holds a current CARC and is contracted with a provider that bills MassHealth, so the visit is covered. Confirm they are licensed to work with Massachusetts residents and follow Massachusetts confidentiality rules. Test the platform once during a calm week, not in the middle of a hard one. Virtual works. The friction it removes is real. The relationship still has to be built deliberately.
Choosing and Working With a Coach: A Treatment Veteran's Checklist
You have done intakes before. You know the questions clinicians ask you. The coaching intake runs the other direction — you should be asking most of the questions, and the answers should be specific.
A short list of what to ask in a first call, and what a good answer sounds like:
Are you CARC-certified, and when does your certification renew? A current coach can answer this in one sentence and tell you who supervises them 2.
How long have you been in your own recovery? MassHealth requires two years minimum to bill the benefit 1. Most coaches will offer more context than the floor.
Are you contracted with a MassHealth provider? If you are a member, this determines whether the work is covered without a separate bill 1.
What kind of recovery experience do you bring? Opioid use disorder, alcohol, stimulants, co-occurring conditions, parenting in recovery, older adult work — fit matters, and specialized tracks like the Older Adult Peer Specialist exist for a reason 13.
What happens when something clinical comes up between us? A solid answer names the referral path — your prescriber, your therapist, a crisis line — and does not blur the scope.
Once you start, give the relationship a real runway. Three or four sessions is not enough to know if a coach is your coach. Six to eight, with honest feedback in between, usually is. Tell them what is landing and what is not. A good coach wants that information and will adjust. If after two months it still feels off, switching is not a setback — it is the same matching work clinicians ask you to do with therapists.
What the Research Supports — and What It Doesn't
Here is the honest version, because you have earned it. Peer recovery support is one of the most active areas of recovery research right now, and the picture is encouraging in some places and still forming in others.
A 2025 systematic review of peer recovery support services and recovery coaching for substance use disorder pulled together the studies done to date and found meaningful signals across engagement, retention, and recovery capital — and also documented significant heterogeneity across peer models and outcome measures 11. SAMHSA has long made the same caveat: the role is well-defined, the evidence base is growing, and more rigorous studies are still needed 10. That is not a reason to skip peer coaching. It is a reason to hold realistic expectations.
Building Your Aftercare Stack in the Next 30 Days
You do not have to assemble all of this at once. A 30-day plan is enough to put the bones in place.
Week one, confirm your clinical layer is steady — therapist, prescriber, any medication you take. That is the foundation everything else leans on.
Week two, call MassHealth or your MCO and ask which contracted providers offer Recovery Coach Services in your area; the benefit is there if you are a member 1. Have a first conversation with one or two coaches using the questions from the checklist above.
Week three, walk into a Peer Recovery Support Center near you, or join a virtual session through a Recovery Learning Community if geography is the obstacle 5, 6.
Week four, write down what is working and what is not, and tell your coach and your clinician honestly.
That is the stack. Coach, community, clinical care. If you are in Massachusetts and want a virtual entry point that holds the peer and clinical layers together, Pathfinder Recovery is one option built for exactly this stretch. Whatever route you take, the next step is small and concrete — and that is enough.
Frequently Asked Questions
Is a peer recovery coach the same as a therapist or sponsor?
No. A therapist provides licensed clinical care — diagnosis, psychotherapy, treatment planning. A sponsor is a mutual-aid relationship inside a specific fellowship like AA or NA, usually unpaid and informal. A peer recovery coach is non-clinical support from someone with lived recovery experience, working under a defined credential and scope 10. Different roles, different rules, different parts of your week.
Does MassHealth cover peer recovery coaching in Massachusetts?
Yes. If you are a MassHealth member seeking to achieve or maintain recovery from a substance use disorder, Recovery Coach Services are a covered benefit through your MCO, ACPP, or the Behavioral Health vendor 1. The coach has to be qualified and contracted with a provider that bills the benefit. Call your plan and ask which contracted providers offer Recovery Coach Services in your area.
How do I verify a coach is CARC-certified before I start working with them?
Ask directly in your first call. A current coach can tell you their certification status, when it renews, and who supervises them 2. If they hedge or cannot name a supervisor, that is a signal. You can also ask which Massachusetts organization issued the credential and whether their employer or contracting agency keeps documentation on file. Verifying is a normal part of vetting, not an insult.
Can I work with a peer coach virtually if I live in Western or Central MA?
Yes, and for many people in rural parts of the state it is the only realistic way to keep the relationship going. The coaching work — goal-setting, lived-experience support, weekly check-ins — translates well to video and phone 10. Confirm the coach holds a current CARC, is contracted with a MassHealth-billing provider if you want coverage, and follows Massachusetts confidentiality rules for telehealth.
What's the difference between a peer recovery support center and a Recovery Learning Community?
Peer Recovery Support Centers are free, drop-in, peer-led spaces specifically for people in recovery from substance use 5. Recovery Learning Communities are peer-run networks offering self-help, information and referral, advocacy, and training, with roots in the mental health peer tradition and substantial substance use overlap 6. If you have co-occurring conditions, RLCs often hold that intersection well. Many people use both.
Should I use peer coaching instead of clinical aftercare, or alongside it?
Alongside. Peer coaching is non-clinical by design — it does not replace therapy, medication management, or crisis care 10. Clinical aftercare handles what is happening inside your nervous system. Peer coaching handles what is happening in your week. Most treatment veterans in Massachusetts who stay connected past month nine have both layers running together, plus a community space they can walk into.
No items found.
[{"@context":"https://schema.org","@type":"BlogPosting","headline":"Peer Coaching Options in MA for Real-World Recovery","description":"Explore certified peer coaching options in MA to support recovery with MassHealth benefits, virtual access, and tailored local resources.","publisher":{"@type":"Organization","name":"Pathfinder Recovery"},"mainEntityOfPage":{"@type":"WebPage","@id":"https://www.pathfinder-recovery.com"}},{"@context":"https://schema.org","@type":"MedicalWebPage","headline":"Peer Coaching Options in MA for Real-World Recovery","description":"Explore certified peer coaching options in MA to support recovery with MassHealth benefits, virtual access, and tailored local resources.","mainEntityOfPage":{"@type":"WebPage","@id":"https://www.pathfinder-recovery.com"}},{"@context":"https://schema.org","@type":"FAQPage","mainEntity":[{"@type":"Question","name":"Is a peer recovery coach the same as a therapist or sponsor?","acceptedAnswer":{"@type":"Answer","text":"No. A therapist provides licensed clinical care \u2014 diagnosis, psychotherapy, treatment planning. A sponsor is a mutual-aid relationship inside a specific fellowship like AA or NA, usually unpaid and informal. A peer recovery coach is non-clinical support from someone with lived recovery experience, working under a defined credential and scope. Different roles, different rules, different parts of your week."}},{"@type":"Question","name":"Does MassHealth cover peer recovery coaching in Massachusetts?","acceptedAnswer":{"@type":"Answer","text":"Yes. If you are a MassHealth member seeking to achieve or maintain recovery from a substance use disorder, Recovery Coach Services are a covered benefit through your MCO, ACPP, or the Behavioral Health vendor. The coach has to be qualified and contracted with a provider that bills the benefit. Call your plan and ask which contracted providers offer Recovery Coach Services in your area."}},{"@type":"Question","name":"How do I verify a coach is CARC-certified before I start working with them?","acceptedAnswer":{"@type":"Answer","text":"Ask directly in your first call. A current coach can tell you their certification status, when it renews, and who supervises them. If they hedge or cannot name a supervisor, that is a signal. You can also ask which Massachusetts organization issued the credential and whether their employer or contracting agency keeps documentation on file. Verifying is a normal part of vetting, not an insult."}},{"@type":"Question","name":"Can I work with a peer coach virtually if I live in Western or Central MA?","acceptedAnswer":{"@type":"Answer","text":"Yes, and for many people in rural parts of the state it is the only realistic way to keep the relationship going. The coaching work \u2014 goal-setting, lived-experience support, weekly check-ins \u2014 translates well to video and phone. Confirm the coach holds a current CARC, is contracted with a MassHealth-billing provider if you want coverage, and follows Massachusetts confidentiality rules for telehealth."}},{"@type":"Question","name":"What's the difference between a peer recovery support center and a Recovery Learning Community?","acceptedAnswer":{"@type":"Answer","text":"Peer Recovery Support Centers are free, drop-in, peer-led spaces specifically for people in recovery from substance use. Recovery Learning Communities are peer-run networks offering self-help, information and referral, advocacy, and training, with roots in the mental health peer tradition and substantial substance use overlap. If you have co-occurring conditions, RLCs often hold that intersection well. Many people use both."}},{"@type":"Question","name":"Should I use peer coaching instead of clinical aftercare, or alongside it?","acceptedAnswer":{"@type":"Answer","text":"Alongside. Peer coaching is non-clinical by design \u2014 it does not replace therapy, medication management, or crisis care. Clinical aftercare handles what is happening inside your nervous system. Peer coaching handles what is happening in your week. Most treatment veterans in Massachusetts who stay connected past month nine have both layers running together, plus a community space they can walk into."}}]}]
Pathfinder Recovery offers in-home addiction and mental health treatment that fits your life — not the other way around.From at-home detox and MAT to virtual IOP and peer support, our licensed clinicians bring evidence-based care to you through secure telehealth.
The Pathfinder Recovery App and Smart Ring keep your care team connected to your progress between sessions — monitoring sleep, stress, and recovery milestones in real time.It’s proactive, private, and personalized — so support is always within reach.
Discover how Mind Body Therapy at Pathfinder Recovery offers holistic, stigma-free healing from home—supporting mental balance, emotional wellness, and lasting recovery.
Find compassionate, evidence-based care with Pathfinder’s Virtual MAT Support—online medication-assisted treatment that supports stable, lasting recovery.
Understand the key differences between therapy vs counseling to choose the right approach for addressing mental health and life challenges effectively.