
How to Get Suboxone Treatment Near Me (From Home)
Get Suboxone treatment near me from home with Pathfinder Recovery. Navigate telehealth, insurance, and virtual care for smooth, safe recovery.
April 22, 2026


Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
You already know the hardest day isn't the one you check in. It's a Tuesday about three weeks after discharge, when the structure is gone, the group chat has quieted down, and you're staring at a full week that nobody else is going to organize for you. If you've done this before, you know that feeling. And you know how quickly it can slide.
New Hampshire makes that slide steeper than most states. The CDC pegs the state's drug overdose death rate at 21.6 per 100,000 people, tied to 293 deaths in the most recent reporting year. That number sits above the current national picture, and it doesn't spread evenly. It concentrates in the places where continuing support is thinnest — smaller towns, longer drives, one prescriber for a whole county.4,10
So the useful question, if you've already been through detox or a residential stay or an IOP, isn't which program to enroll in next. It's what you build around yourself in the weeks after you walk out. Peer support, a prescriber who takes your calls, housing that doesn't test you every night, a therapist who sees you on a screen because the closest office is 40 miles away. That combination — assembled deliberately, kept intact through bad weeks — is what continuing care actually looks like here. The rest of this guide is about how to put it together.
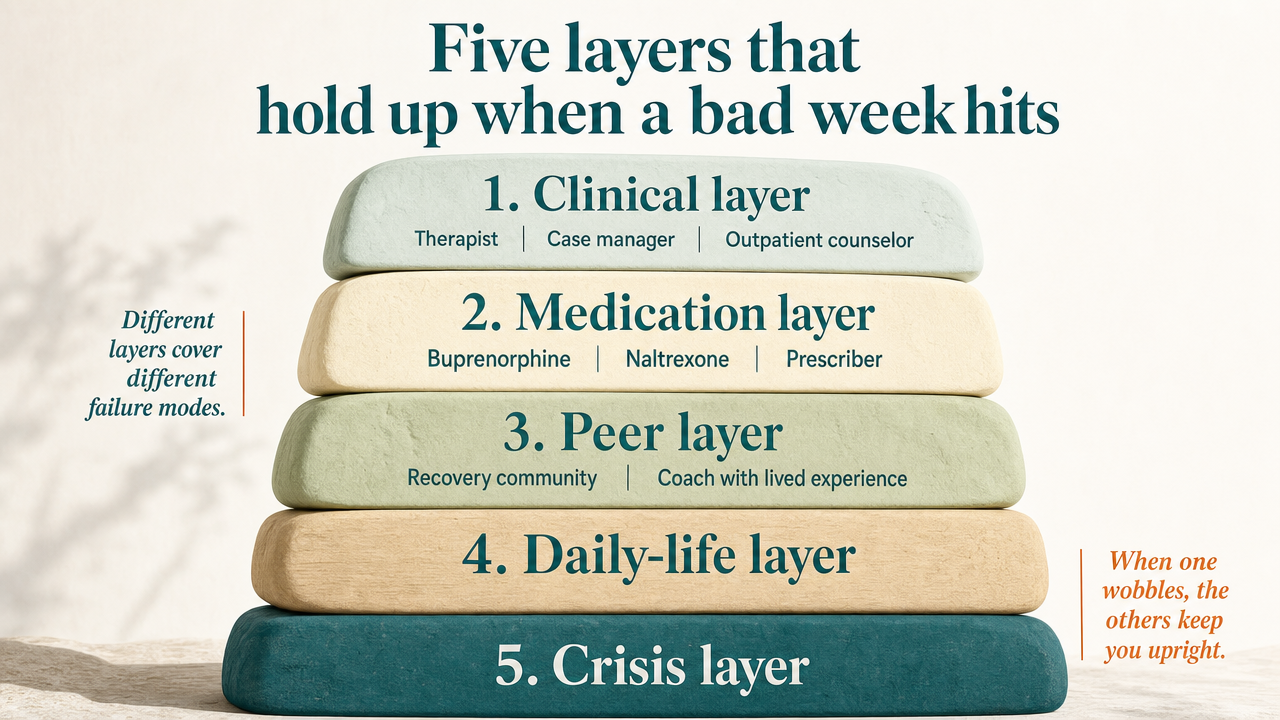
Think of continuing care as five layers stacked together, not a single program you sign up for. Each layer covers a different failure mode, and when one wobbles, the others keep you upright.
The clinical layer is your therapist, your case manager, your outpatient counselor — the people paid to track how you're actually doing. Under New Hampshire's Medicaid rules, this layer can include case management, therapy, and other evidence-based recovery supports coordinated alongside SUD care. The medication layer is buprenorphine, naltrexone, or whatever your prescriber has you on, plus the person who writes the script and adjusts it when life shifts. NH covers medication-assisted treatment as part of that same set of reimbursable services.7
The peer layer is the recovery community organization, the coach with lived experience, the meeting you actually attend. The housing layer is where you sleep — ideally a certified recovery residence tracked through the state's voluntary registry. And the family and work layer is the practical scaffolding: who knows what, who covers the kids on a hard afternoon, how your schedule holds.9
A bad week doesn't take out all five at once. That's the whole point of building it this way.
You can't build all five layers in the same week, and if you try, you'll burn out by Friday. Order matters.
Lock in medication first if you're on it. A confirmed prescriber, a filled script, and a plan for the next refill — before anything else. A gap here is the fastest way back to where you started, and everything else in the stack loses value if this layer breaks.
Housing comes next, because it decides what your Tuesday night actually looks like. If you're going home to a place that isn't safe for early recovery, sort that before your first therapy appointment, not after. A certified recovery residence listed through the state registry is worth the extra calls.9
Then clinical — an outpatient therapist or case manager with a standing weekly slot. Then peer support, which you'll lean on more than you expect. Family and work conversations come last, once you have something concrete to tell people about how you're structuring the next 90 days.
If you already have one or two layers from a previous round, keep them. Don't rebuild from scratch. Add what's missing.
Here's what most people don't realize until they try to book something: New Hampshire Medicaid does cover ongoing recovery support, not just acute treatment. The rules are spelled out in the state's administrative code, and if you know what to ask for, you can build most of the clinical layer without paying out of pocket.
Under He-W 513.05, the reimbursable list includes case management, medication-assisted treatment, individual and group therapy, and other evidence-based recovery supports coordinated alongside SUD care. Case management is the one people skip and shouldn't. A case manager is the person who calls the pharmacy when your prescription gets stuck, who knows which outpatient program has an opening this week, who follows up when you miss an appointment instead of dropping you from the roster.7
What the code doesn't cover as neatly: transportation to appointments, help with rent, childcare during your group sessions. Those gaps are real, and they're often the reason people fall off the schedule. Ask your case manager what workarounds exist in your region before you assume something isn't possible. A ride voucher or a shifted appointment time can be the difference between showing up for six months and stopping in week three.
You've probably sat across from someone in a clinical setting who clearly hadn't done this work long. You know the feeling. New Hampshire's provider rules give you a way to check credentials before you get to that appointment.
He-W 513.04 sets the minimum for anyone billing Medicaid for SUD services. Counselors delivering the work must have completed at least one year in the field under the supervision of a Master Licensed Alcohol and Drug Counselor (MLADC) or a licensed mental health provider. That's the floor. Many good clinicians go well above it, but nobody billing the state should be below it.8
When you call a provider, ask two things directly: who supervises the clinician you'd be seeing, and what their MLADC or licensure credential is. If the answer is vague, that tells you something. If the front desk can name the supervising clinician without pausing, that also tells you something. You're a peer to the process at this point — you've earned the right to ask.
The reason NH Medicaid covers as much of the recovery stack as it does comes down to a Section 1115 demonstration — a federal waiver that lets the state test approaches beyond standard Medicaid benefit limits. It's the legal machinery behind most of the continuing care you can access here.1,3
CMS extended the demonstration in June 2024, and the extension did something worth knowing about. It kept the existing authorities for residential and outpatient SUD services and added limited coverage for certain reentry services for people leaving incarceration. If you or someone you're supporting is coming out of jail or prison, that's a meaningful change — Medicaid can now cover specific services in the window around release, which used to be a hard cliff.2
The waiver isn't permanent. Extensions have to be renewed, and evaluation questions about long-term outcomes and funding remain live. For your purposes right now, that means two things: the services are real and reimbursable today, and it's worth locking in a case manager who tracks changes, so you're not the last to know when something shifts.3
Medication-assisted treatment works when it's boring. A steady dose, a script that gets refilled on time, a prescriber who returns messages within a day or two. That's the goal. Drama in this layer — a lapsed prescription, a pharmacy that doesn't stock your medication, a provider who leaves the practice — is what puts people back in the emergency department.
Buprenorphine and naltrexone are both covered under New Hampshire Medicaid as part of the same set of reimbursable SUD services that includes counseling and case management. That matters because it means your medication and your therapy can sit inside one coordinated plan instead of being billed and tracked separately. If your prescriber and your therapist aren't talking, ask your case manager to loop them in. That's part of what case management is for.7
Two practical moves protect this layer. First, know your refill date before you need it, and set a reminder three days out — not the morning of. Second, ask your prescriber what happens if you miss a dose, a week, or a month. Get the honest answer now, when you're stable, not later when you're not. A prescriber who won't have that conversation is telling you something about how they'll handle a hard week.
Your therapist has a caseload. Your prescriber has a schedule. Neither of them is going to text you back at 9:47 on a Saturday night when you're sitting in a parking lot trying to decide what to do next. A peer is.
That's the honest difference. Recovery community organizations and certified peer support specialists in New Hampshire fill a gap the clinical system isn't built to cover — the unstructured hours, the messy calls, the ride to a meeting when your car won't start. Peers have been where you are. They know what an early Tuesday actually feels like, and they aren't billing for the conversation.
What a good peer relationship gives you: a person who will show up at a meeting because you said you'd be there, someone who can walk you into a first appointment when the front-desk conversation feels impossible, and a check-in that doesn't require you to perform being fine. What it doesn't give you: therapy, medication, or a diagnosis. Peers work alongside your clinician, not instead of one. If someone is offering peer support as a replacement for clinical care, that's a signal to look elsewhere.
Practical move — build the peer layer before you need it. Introduce yourself to a recovery community organization while you're stable, not in the middle of a hard night. A relationship you already have holds up better than one you're trying to start at 9:47.
New Hampshire keeps a registry of certified recovery houses, and the state's own rule tells you exactly what it is and isn't. Under He-A 305.01, the registry's stated purpose is to establish a voluntary list of operators and a process for receiving and acting on complaints. Read that word again: voluntary. Any house you're considering can choose to be on it, or not.9
That matters for you in two directions. A residence on the registry has agreed to a baseline and has a complaint channel behind it — that's real, and it's worth asking about before you sign anything. A residence not on the registry isn't automatically bad, but you lose the state-tracked complaint pathway if things go sideways, and you're relying entirely on the operator's word about how the house runs.
When you tour or call a house, ask three things: are you on the state registry, what happens when a resident returns to use, and who owns the building. Vague answers to any of those aren't disqualifying on their own, but pattern them together. A house that can't tell you its return-to-use policy is a house that hasn't thought about one.
Sober living and licensed residential treatment aren't the same thing, and the credentials you're looking for differ. If you're evaluating a residential SUD facility — not a peer-run recovery house — the state's rule is that licensure through the Department of Health and Human Services is required to operate, and accreditation is not required.6
What that means in practice: a facility can be legally operating and still hold no third-party accreditation from bodies like CARF or Joint Commission. Neither answer is automatically a red flag, but they tell you different things. Licensure means the state signed off on the basics. Accreditation, when a facility has it, means an outside body reviewed the clinical work against a national standard.
Ask directly: what license does the facility hold, and are you accredited by anyone. If the answer to the second one is no, ask why. A confident, specific answer is fine. A defensive one is information too.
If you live in Coos County, your recovery math is different from someone in Nashua. The closest MLADC-supervised outpatient program might be 45 minutes away in decent weather. The nearest peer meeting that isn't in a church basement on Tuesday nights might not exist. And the prescriber who took your last refill call might be the only one within an hour who takes new patients this quarter. That's not a personal failing. That's geography.
The rural piece isn't hypothetical. Research on opioid mortality in northern New England found NH's opioid fatality rate hit 31.3 per 100,000 in 2015, with rural counties carrying disproportionate weight because of thinner healthcare access and longer distances to care. Those structural gaps didn't disappear when the national picture started improving. U.S. overdose deaths dropped from 110,037 in 2023 to an estimated 80,391 in 2024 — a 26.9% decline. That's real progress, and it makes the leverage point clearer: holding those gains for the long haul depends on continuing care, not just crisis response. Nobody stays alive on naloxone alone.5,11
Virtual continuing care is where the geography argument stops being theoretical. A therapy session over video from your kitchen is a full session, not a lesser one. A prescriber visit by phone counts for your medication management. A peer check-in on an app on Sunday night is a real check-in. If the closest in-person option is a 90-minute round trip you'll skip after week four, the honest question isn't whether virtual is as good as in-person. It's whether you'll actually show up.
You have not failed at recovery because your county lacks providers. You are working with what the map gives you. Virtual care lets the map matter less.
Nobody in your life needs the full clinical picture. But somebody needs to know enough to be useful on a hard day, and figuring out who that is takes some thought.
Start with one person at work and one person at home. At work, that's usually a manager or HR contact who knows you have medical appointments on Wednesday afternoons — not why, not the diagnosis, just that the schedule matters and it's not negotiable. At home, that's the partner, sibling, parent, or roommate who knows what medication you take, where the prescriber's number is, and what to do if you go quiet for two days. Keep the circle small on purpose. More people knowing does not equal more support.
Then protect the calendar. Recovery appointments are not the thing you move when work gets loud. They are the thing work moves around, because if this layer collapses, the paycheck follows within a few months anyway. A standing therapy slot, a monthly prescriber check-in, and a recurring peer call belong on the calendar the same way a mortgage payment does — automatic, non-negotiable, discussed only when something bigger is genuinely on fire.
One quiet win to celebrate: a week where you kept every appointment and told nobody about it. That's the layer working.
A return to use is not the end of your recovery. It is information. What you do in the next three days matters more than what happened in the last three hours.
Hour one to twelve: call your prescriber or your case manager. Not your sponsor, not a friend — the clinical person first, because medication decisions are time-sensitive. If you're on naltrexone or buprenorphine, the dosing math after a return to use is not something to figure out alone. Under NH Medicaid, case management sits inside the same coordinated set of services as your MAT, which is exactly what that layer is designed for. Use it.7
Day one to three: keep every appointment already on your calendar. Do not cancel therapy because you feel like you failed at it. That's the appointment you need most. Tell your peer contact. Tell the one person at home who's supposed to know. If you're in a certified recovery residence, be honest with the operator — the state registry's complaint process exists partly because good houses handle returns to use with a plan, not a bag on the porch.9
What not to do: disappear, restart a residential stay reflexively, or decide alone that you have to rebuild the whole stack. A return to use usually means one layer wobbled, not five. Find which one, shore it up, and keep going. That's the work.
Ninety days is long enough to build something real and short enough to actually finish. Here's what a working plan looks like when you already know the vocabulary.
Weeks 1 to 2. Confirm your prescriber, your script, and your next refill date. Book a standing weekly therapy slot with a provider whose clinician credentials you actually asked about. If your housing situation is shaky, this is the two-week window to fix it — call houses on the state registry, ask the three questions, sign only when the answers hold up.8,9
Weeks 3 to 6. Add the peer layer. One recovery community organization, one person you have a real number for. Ask your case manager to coordinate your therapy, medication, and any additional recovery supports inside one Medicaid-covered plan rather than three unconnected ones. Have the small conversation with one person at work and one person at home.7
Weeks 7 to 12. Protect what you built. Keep the calendar. Notice which layer wobbles first when you get tired — that's the one to shore up next quarter.
You have done harder things than this. Pathfinder Recovery works with people across New Hampshire doing exactly this kind of assembly, virtually, one appointment at a time. Keep going.
Yes, and more than most people assume. Under He-W 513.05, NH Medicaid covers case management, medication-assisted treatment, individual and group therapy, and other evidence-based recovery supports coordinated alongside SUD care. The Section 1115 waiver is what makes this reach possible, and its 2024 extension added limited reentry services for people leaving incarceration.2,7
Start with the state's voluntary registry of certified recovery houses, which exists to track operators and handle complaints. Ask three questions before signing: are you on the registry, what happens when a resident returns to use, and who owns the building. Registry listing isn't required to operate, so a house not on it isn't automatically bad — but you lose the complaint channel.9
It's real. A therapy session over video counts as a full session, and a prescriber visit by phone counts for your medication management. In rural New England, opioid mortality has hit disproportionately hard partly because in-person care is so far away — NH's 2015 opioid fatality rate reached 31.3 per 100,000. Virtual care lets you show up weekly instead of skipping after mile 45.5
Under He-W 513.04, any counselor billing NH Medicaid for SUD services must have completed at least one year in the field under supervision of a Master Licensed Alcohol and Drug Counselor (MLADC) or a licensed mental health provider. Ask directly who supervises the clinician you'd see and what their credential is. A confident, specific answer is the floor. Vague answers tell you to keep looking.8
Usually no. A return to use often means one layer of your continuing care wobbled, not five. Call your prescriber or case manager first, because medication dosing decisions are time-sensitive — case management sits inside the same coordinated Medicaid-covered set as your MAT for exactly this reason. Keep the appointments already on your calendar. Restarting residential reflexively skips the diagnostic work of finding which layer broke.7
Peers cover the unstructured hours a clinician can't — the Saturday night text, the ride to a meeting, the walk into a first appointment. Clinicians provide therapy, medication, and diagnosis. They aren't interchangeable. NH Medicaid coordinates both alongside SUD care under one plan when you ask for it. Most people who hold recovery long-term have both. If someone offers peer support as a replacement for clinical care, look elsewhere.7
April 22, 2026

November 6, 2025

May 4, 2026