
Virtual Holistic Addiction Treatment Options in NH
Explore how holistic addiction treatment virtual NH programs combine therapy, MAT, and peer support to improve access and recovery outcomes.
May 4, 2026


Written and reviewed by the leadership team at Pathfinder Recovery, including licensed medical and clinical professionals with over 30 years of experience in addiction and mental health care.
It's 7:14 a.m. You're already three emails deep, the coffee is still too hot, and there's a quiet question in the back of your mind that has been there for weeks: how do I actually do something about this without blowing up my schedule?
You're not looking for a dramatic intervention. You're looking for something that fits between a 9 a.m. status call and the school pickup, something that doesn't require explaining a two-hour gap on your calendar or being seen in a clinic parking lot two towns over. You want help, and you want to keep your job, your license, and the parts of your life that are working.
That's a reasonable place to start. It's also the place where most working professionals in Connecticut quietly land before they ever pick up the phone.
Virtual recovery support has changed what's possible here. Peer coaching check-ins on a lunch break. An intensive outpatient group on Tuesday and Thursday evenings. Medication management visits that fit between meetings. Co-occurring care for the anxiety or depression riding alongside the drinking or the pills. None of it requires you to disappear from your own life.
This guide walks through what that actually looks like in CT — what the care channels do, how they fit together, and how to protect your schedule and your privacy while you start.
You're not imagining the weight of this. Connecticut has been carrying a heavier overdose burden than the country as a whole, and that fact shapes why so many working people in the state are quietly looking for care that doesn't require them to stop their lives.
In 2023, Connecticut's age-adjusted unintentional drug-induced mortality rate was 33.3 per 100,000 residents, compared to a national rate of 29.1 per 100,000 1. The state's own health department puts it bluntly: a Connecticut resident is now more likely to die of an unintentional drug overdose than in a motor vehicle crash 1. That's the public-health backdrop behind every late-night search for help.
You probably already feel some version of this in your own circle. A colleague who suddenly took leave. A neighbor's adult son. A funeral that wasn't supposed to happen. The numbers describe a pattern you've likely seen up close.
What that means for you, practically, is two things. One, the urgency you feel about doing something — even something small — is reasonable. The problem isn't waiting for a perfect moment. Two, the state has been responding, and that response includes building out remote and outpatient options specifically because the old model of clinic-only, business-hours-only care wasn't reaching enough people in time. Virtual access isn't a side door. It's a deliberate part of how Connecticut is trying to close the gap.
Here's something worth sitting with before you read another word: you are not unusual. The Connecticut-specific estimates from the 2022–2023 National Survey on Drug Use and Health put past-month illicit drug use among adults 18 and older at roughly 19.92%, and past-year marijuana use at about 25.37%, with confidence intervals around those modeled figures 15. Roughly one in five CT adults reports past-month illicit drug use. That's a lot of people going to work on Monday.
Most of them are not in treatment. Most are functioning, more or less, and managing the gap between what they show at work and what they do at home. Some are noticing the gap getting harder to maintain.
If that sounds familiar — the careful timing, the calendar arithmetic, the running mental tally of how much, how often, how visible — it doesn't mean you've failed at something. It means you're a person living in a state where a meaningful share of your peers are doing some version of the same math. The fact that you're now looking for support is the part that's different.
The treatment system in Connecticut was built assuming most people who need help won't reach for it. You reaching for it, even tentatively, even by reading a webpage at 11 p.m., is the unusual move. Everything from here is just figuring out what kind of help fits.
Short answer: yes, and it's not a workaround. It's where a large share of the state's behavioral health infrastructure now lives.
A UConn Health report identified 282 behavioral health facilities serving Medicaid beneficiaries in Connecticut, and 65% of them provide telehealth services 11. That's nearly two out of three providers in the state's safety-net system offering remote care as a standard option — not a pandemic-era band-aid that quietly disappeared. Commercial insurance networks in Connecticut have followed similar patterns, with most major carriers covering telehealth-delivered SUD and behavioral health services at parity with in-person visits.
What that means for you, sitting at your desk: when you start calling around or filling out intake forms, virtual is not the strange request. It's the default option at most places worth considering. You will not have to argue for it.
There's also a clinical evidence base behind this shift. Federal guidance from SAMHSA on telehealth for SUD and serious mental illness lays out which modalities work for which populations, including induction and maintenance on medications for opioid use disorder, individual and group therapy, and care coordination 7. National data on telemedicine adoption in SUD and mental health treatment shows sustained, not transitional, use 8. Translation: clinicians and regulators have moved past the question of whether this works.
Your job isn't to validate the channel. Your job is to find the right mix inside it.
This is the one most people get wrong before they start, so let's clear it up.
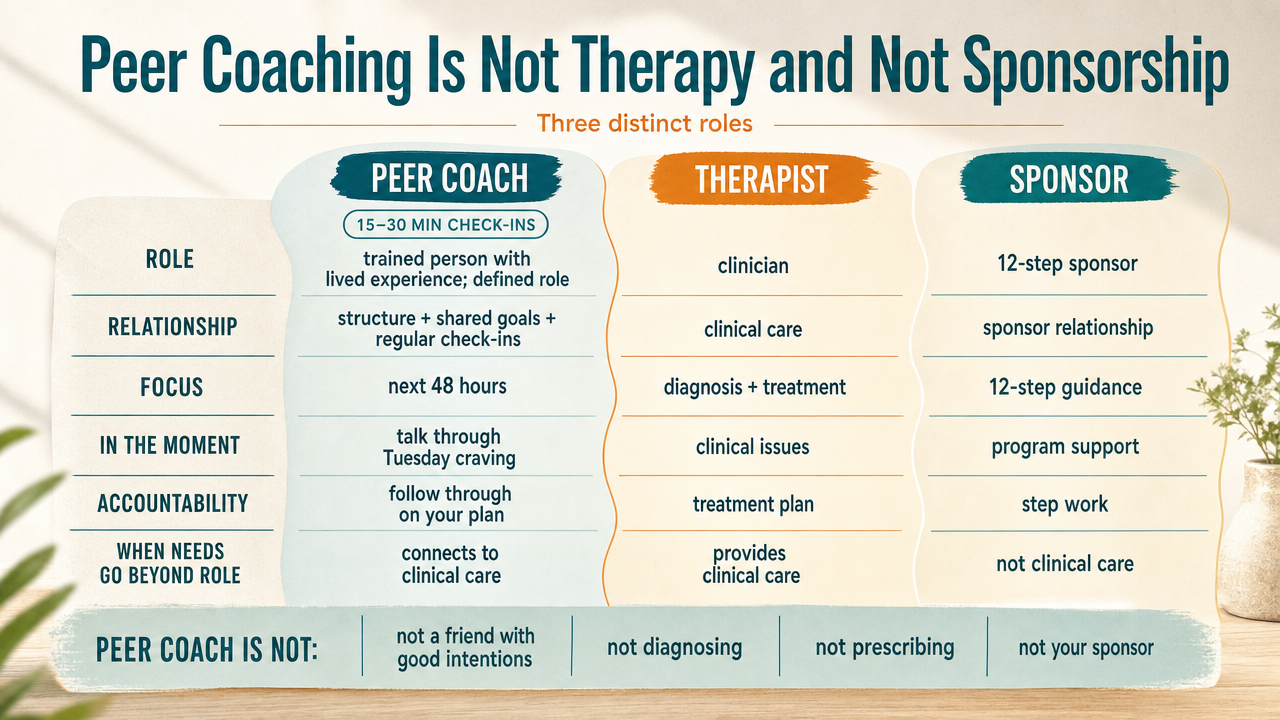
A peer recovery coach is a trained person who has lived through their own substance use disorder and now works in a defined role helping others. Not a friend with good intentions. Not a 12-step sponsor. Not a clinician. The coaching relationship has a structure, goals you set together, and regular check-ins that often run 15 to 30 minutes — short enough to fit before a 9 a.m. or during a lunch break.
What a coach actually does: helps you think through the next 48 hours, talks through a craving that hit on a Tuesday afternoon, holds you accountable to whatever you said you'd do, and connects you to clinical care when something is above their pay grade. They are not diagnosing you. They are not prescribing anything. They are not your sponsor running you through a program of recovery from a specific tradition.
Therapy is different work — slower, focused on the patterns underneath the using. Sponsorship, if you choose that path, is a peer relationship inside a mutual-help fellowship, unpaid and outside any clinical system. Coaching sits in between, with professional boundaries and lived experience in the same room.
For a working professional, the value is often the cadence. You don't have to be in crisis to get on a call.
These are the three clinical layers that do most of the heavy lifting, and each one answers a different question.
A virtual Intensive Outpatient Program (IOP) is a structured group treatment that typically runs three evenings a week, around three hours per session, for eight to twelve weeks. You log in from home. The group is small, the curriculum is built around relapse prevention, coping skills, and the actual mechanics of staying in recovery while life keeps happening. Evening scheduling exists because the people who need IOP usually have jobs. If you've been picturing a daytime program you'd have to take leave for, that's a different level of care.
Individual therapy, virtual or otherwise, is the 50-minute weekly conversation with a licensed clinician — typically using approaches like cognitive behavioral therapy, motivational interviewing, or mindfulness-based work. This is where you do the slower work on what's driving the use, what trauma or pattern keeps surfacing, what you actually want your life to look like.
Medication management is a shorter, more clinical visit — often 20 to 30 minutes — with a prescriber who handles medications for opioid or alcohol use disorder, like buprenorphine, naltrexone, or Suboxone. SAMHSA's evidence-based guidance covers induction and maintenance for these medications via telehealth, including for serious mental illness and SUD overlap 7. National telemedicine data shows this is now standard practice, not an exception 8.
Most people don't use all three at once. You build the stack you need.
If you're using something to take the edge off something else, you already know this part.
Anxiety that won't let you sleep without a drink. Depression that makes the pills feel like the only thing that works. Old trauma that surfaces when you're sober and goes quiet when you're not. This is the co-occurring picture, and it's common — common enough that treating the SUD without addressing what's riding alongside it tends to fall apart within months.
Virtual SUD programs that include co-occurring mental health support handle this differently than primary mental health care. The framing matters. The work happens alongside your substance use treatment — your therapist and prescriber know the whole picture, the anxiety treatment is built into the same plan as the recovery work, and you're not bouncing between two unconnected systems trying to explain yourself twice. SAMHSA's clinical guidance explicitly addresses integrated telehealth models for people with SUD and co-occurring mental health conditions 7.
If your primary issue is a standalone mental health condition with no substance use component, that's a different referral. But if the two are tangled together — and for a lot of working professionals quietly managing both, they are — integrated virtual care is built for exactly this. You don't have to pick which problem to treat first.
Forget the brochure version. Here's what a working week can actually hold when you're stacking virtual care around a real job.
That's about four hours of structured care across a 40 to 50 hour workweek. Nobody on your team knows. Nothing shows on your shared calendar except blocks labeled however you label them. The work is real and so is the rest of your life.
This is the part that keeps a lot of working professionals stuck. Not the cost. Not the time. The question of who finds out.
Start with the floor: federal law treats SUD treatment records as among the most protected health information in the country. 42 CFR Part 2 sits on top of HIPAA and limits how a treatment program can share that you were ever a patient — even with other clinicians, even with your primary insurance, without your specific written consent. That doesn't mean nothing leaves the building. It means the rules for what can leave, and to whom, are unusually strict.
What your insurance company actually sees if you use your benefits: dates of service, diagnosis codes, procedure codes, and the provider's name. They do not see your session notes. They do not see what you said in group on Tuesday. Your employer, if you're on a group plan, does not see individual claims — they see aggregate cost data for the whole population.
Licensure boards are the sharper question. In most professions and most states, voluntarily seeking treatment for a substance use disorder is not a reportable event. What triggers a board is impairment on the job, a DUI, a diversion incident, a malpractice claim — not the act of getting help. Several states, Connecticut included, run physician health and lawyer assistance programs precisely to keep voluntary, early treatment confidential and separate from disciplinary tracks. If you're worried about your specific board's reporting rules, ask the program's intake team directly before you sign anything. They've answered that question hundreds of times.
Federal parity law requires commercial health plans to cover SUD treatment on the same terms as other medical care. In practice, most Connecticut commercial plans — Anthem, Cigna, Aetna, UnitedHealthcare, ConnectiCare — cover virtual IOP, individual therapy, medication management, and peer support, often with the same copay structure as an in-person visit.
HUSKY Health, Connecticut's Medicaid program, covers virtual SUD and behavioral health services as a standard benefit. That coverage is one reason the 65% telehealth adoption rate among Medicaid-serving facilities matters 11— the payment side caught up to the delivery side.
Before you commit to a provider, ask three things: Is the program in-network with your specific plan? What's the per-session or per-week out-of-pocket cost after your deductible? Do they bill insurance directly or do you pay upfront and submit for reimbursement? The answers vary, and a five-minute call saves a billing surprise in week four.
You don't need to interview twelve programs. You need to ask five questions on a single call, listen for the answers, and trust your read.
Trust the call itself as data. If you feel rushed, talked over, or sold to, that's information. If the intake person asks what you're actually dealing with and listens before pitching anything, that's also information. You're not being difficult by paying attention to this. You're choosing carefully, which is exactly the right move.
If part of what's kept you stuck is the sense that virtual recovery is somehow second-tier — the budget version, the thing you settle for if you can't get into a real program — it's worth knowing where Connecticut actually sits.
The state has been deliberately building infrastructure around this. The Opioid Settlement Advisory Committee directs settlement dollars into treatment, harm reduction, and recovery services, with an annualized budget process that prioritizes accessible care 3. The Connecticut Opioid REsponse (CORE) Initiative, anchored at Yale, coordinates prevention, treatment, and harm-reduction work across the state 4. Near-real-time overdose tracking through Yale's data toolbox feeds back into where resources go 5. This is not a fringe corner of the health system. It's where significant public investment is landing.
What that means for you: when you pick up the phone or fill out an intake form for a virtual program, you're stepping into a care channel that clinicians, regulators, and state funders have spent years legitimizing. The skepticism you might be carrying — that this is somehow less serious than driving to a building — is older than the current system.
The first call is still hard. That's a fair reaction, not a weakness. Providers like Pathfinder Recovery exist because the people who answer that call deserve care that fits the life they're trying to keep.
For outpatient SUD care, the clinical evidence supports telehealth as a legitimate delivery channel, not a compromise. SAMHSA's evidence-based guidance covers virtual therapy, group treatment, and medication management for opioid and alcohol use disorder, including for people with co-occurring conditions 7. National telemedicine data shows sustained adoption well beyond the pandemic 8. What matters more than the channel is the mix of services and how consistently you use them.
A peer coach is a trained professional with lived recovery experience who works in short, structured check-ins — often 15 to 30 minutes — focused on accountability and the next 48 hours. A therapist is a licensed clinician doing slower work on patterns underneath the use. A sponsor is an unpaid peer inside a 12-step fellowship. Coaching sits between them, with professional boundaries and lived experience in the same conversation.
Federal law (42 CFR Part 2) protects SUD treatment records more strictly than ordinary medical records. Your employer does not see individual claims on a group plan. In most professions, voluntarily seeking treatment is not a reportable event to a licensing board — what triggers boards is impairment, a DUI, or a diversion incident, not the act of getting help. Ask the program's intake team about your specific board before signing anything.
Yes, in most cases. Federal parity law requires commercial plans to cover SUD treatment on the same terms as other medical care, and the major Connecticut carriers cover virtual IOP, therapy, medication management, and peer support. HUSKY Health covers virtual SUD and behavioral health services as a standard benefit, which is part of why 65% of CT behavioral health facilities serving Medicaid beneficiaries now offer telehealth 11. Confirm in-network status before starting.
Yes. Buprenorphine, Suboxone, and naltrexone can be prescribed and managed through telehealth visits with a CT-licensed prescriber. SAMHSA's clinical guidance covers virtual induction and maintenance for medications used in opioid and alcohol use disorder, including for people with co-occurring mental health conditions 7. Medication management visits typically run 20 to 30 minutes and can fit between work meetings. Your prescriber coordinates refills, side effects, and dose adjustments remotely.
If you're in immediate danger, call 911 or go to an emergency room. For urgent but non-emergency support, SAMHSA's National Helpline is free, confidential, and available 24/7, 365 days a year in English and Spanish at 1-800-662-HELP (4357) 6. The 988 Suicide and Crisis Lifeline also handles substance-related crises. Most virtual programs offer same-day or next-day peer coaching access — ask about after-hours options when you call intake.
May 4, 2026

May 5, 2026

November 6, 2025